Pancreatic and hepatobiliary cancers remain among the most formidable challenges in modern oncology. With five-year survival rates lingering below 10%, these malignancies are often identified only at advanced, incurable stages. For decades, clinicians have searched for reliable, non-invasive biomarkers that could act as an "early warning system." A recent multi-institutional retrospective study, published in Cancers, has shed new light on an old diagnostic player: Gamma-glutamyl transferase (GGT).
The study, which analyzed over 29,000 patients, suggests that while GGT may not be the elusive "magic bullet" for early pancreatic cancer detection, its persistent elevation serves as a vital red flag for a broader spectrum of hepatobiliary and inflammatory diseases.
Main Facts: Redefining the Role of GGT
GGT is a membrane-bound enzyme primarily known for its role in glutathione metabolism—the body’s master antioxidant defense system. While it is standard practice to test GGT during routine liver panels, it is often dismissed as a non-specific marker of alcohol consumption or minor bile duct irritation.
However, the researchers behind this study argued that the traditional "single-point" measurement approach is flawed. By focusing on patients with persistently elevated GGT—defined as levels of at least 65.00 U/L confirmed twice within a 6 to 12-month window—the team identified a distinct group of individuals at significantly higher risk for serious health outcomes.
The core findings reveal that persistent GGT elevation is strongly associated with:
- Cholangiocarcinoma: A threefold increase in risk.
- Hepatocellular Carcinoma (HCC): A twofold increase in risk.
- Pancreatic Inflammatory Diseases: A significant spike in both acute and chronic pancreatitis.
- All-Cause Mortality: A twofold increase in mortality rates over the study period.
Crucially, the study found no statistically significant link between persistent GGT elevation and pancreatic cancer, challenging previous observational studies that suggested a causal connection.
Chronology of Research and Methodology
The study utilized the TriNetX analytics platform, a global federated network providing de-identified electronic medical records. The methodology was designed to move beyond the limitations of cross-sectional snapshots.
- Cohort Definition: The researchers identified 26,136 adults with persistently high GGT and 97,649 with normal GGT levels.
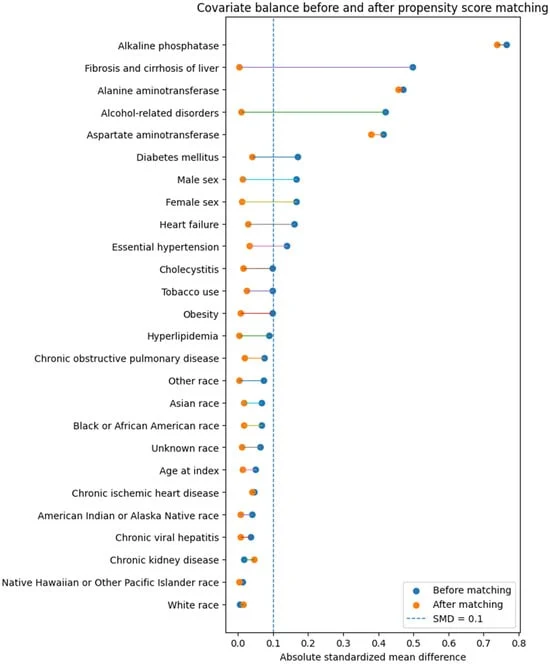
- Propensity Score Matching (PSM): To ensure a fair comparison, the team performed 1:1 matching. This process balanced the groups across age, sex, race, and a comprehensive suite of comorbidities—including hypertension, diabetes, obesity, and known liver disease.
- Outcome Window: The team tracked outcomes between 180 and 1,095 days following the initial index event to exclude immediate diagnostic noise and focus on long-term health trajectories.
- Statistical Validation: Using Cox proportional hazards models, the team calculated hazard ratios to determine the strength of the association between GGT status and subsequent disease events.
Supporting Data: The Magnitude of Risk
The data highlights a clear divergence in health outcomes for those with sustained GGT elevation. In the matched cohorts (14,590 patients in each), the incidence of hepatobiliary malignancy was starkly higher in the elevated GGT group.
Regarding Hepatocellular Carcinoma, the hazard ratio was 2.260. Even after adjusting for baseline liver health, those with high GGT were more than twice as likely to develop primary liver cancer. The data for cholangiocarcinoma was even more striking, showing a hazard ratio of 3.715.
Perhaps most surprising was the correlation with pancreatic inflammatory diseases. The risk of developing acute pancreatitis was more than three times higher in the elevated GGT cohort. The study also documented an association with pancreatic cysts—a finding that, while currently requiring further validation, could open new avenues for risk stratification in gastrointestinal health.

Regarding mortality, the data was unequivocal: the survival probability at the end of the three-year outcome window was 86.95% for the elevated GGT cohort, compared to 93.95% for the normal GGT cohort.
Official Interpretations and Cautions
The research team emphasized that their findings should be viewed as "clinically descriptive and hypothesis-generating." They cautioned that GGT is not a disease-specific biomarker. It is a mirror reflecting a multitude of potential underlying issues: cholestasis, metabolic dysfunction, subclinical inflammation, or the long-term impact of alcohol and medications.
"These findings do not establish GGT as an independent causal risk factor," the authors noted. "Instead, they identify a high-risk group that requires more comprehensive clinical assessment."
The lack of a link to pancreatic cancer in this study, in contrast to earlier research, is attributed to the study’s design. By requiring persistent elevation, the researchers may have filtered out patients who only exhibit metabolic changes in the immediate, rapid-decline phase of pancreatic cancer development. It suggests that if GGT is involved in pancreatic cancer, it is likely part of a complex, dynamic metabolic shift that happens shortly before clinical presentation, rather than a long-term, stable precursor.
Implications for Clinical Practice
The primary takeaway for physicians is that a "high GGT" result should never be ignored, but it should be contextualized.
1. Moving Beyond "Wait and See":
In standard practice, clinicians often re-test GGT after a few weeks to see if it normalizes. The study suggests that if the elevation is persistent, the patient should not be dismissed. It is a marker of an increased "disease burden" that warrants a deeper dive into metabolic health, liver fibrosis, and potential biliary issues.
2. Refined Screening:
While GGT is not a screening tool for pancreatic cancer, it is a powerful indicator of general systemic vulnerability. Patients with persistent elevation who also present with weight loss, abdominal pain, or other non-specific symptoms should be evaluated with higher urgency.
3. Future Research:
The authors advocate for a transition toward "biomarker signatures." Rather than relying on GGT alone, future risk models should combine GGT with inflammatory markers (like CRP), metabolic data (fasting insulin and glucose), and fibrosis scores.
Conclusion
This study serves as a critical reminder that in the age of high-tech diagnostics, traditional laboratory markers still contain vast, untapped reservoirs of information. While persistent GGT elevation is not a direct path to a cancer diagnosis, it is a loud signal from the body that the hepatobiliary and metabolic systems are under chronic stress. By treating this enzyme not just as a "liver test," but as a prognostic indicator of systemic health, clinicians can better identify patients who need early intervention to prevent the progression of severe, life-limiting diseases.
As the authors concluded, the focus must now shift to large-scale prospective studies that track these GGT trajectories over time, helping to move from passive observation to proactive, preventative care.