Since the inception of the Affordable Care Act (ACA) in 2010, few policy mechanisms have transformed the American healthcare landscape as profoundly—or as controversially—as the expansion of Medicaid. Designed as a cornerstone of the ACA’s promise to reduce the number of uninsured Americans, the expansion was intended to provide a safety net for low-income adults who previously fell into a "coverage gap." Today, as the policy enters its second decade, the United States remains deeply divided by a geographic patchwork of coverage, where a citizen’s access to healthcare often depends more on their zip code than their health needs.
Main Facts: Defining the Expansion Landscape
At its core, the Medicaid expansion represents a federal-state partnership designed to extend coverage to nearly all adults with incomes up to 138% of the Federal Poverty Level (FPL). For the 2025 calendar year, this threshold translates to an annual income of $21,597 for an individual.
To incentivize participation, the federal government initially covered 100% of the costs for the expansion population, gradually phasing down to a permanent 90% federal matching rate (FMAP). This financial structure was crafted to relieve state budgets of the heavy burden of caring for the uninsured, shifting the fiscal responsibility largely to the federal ledger.
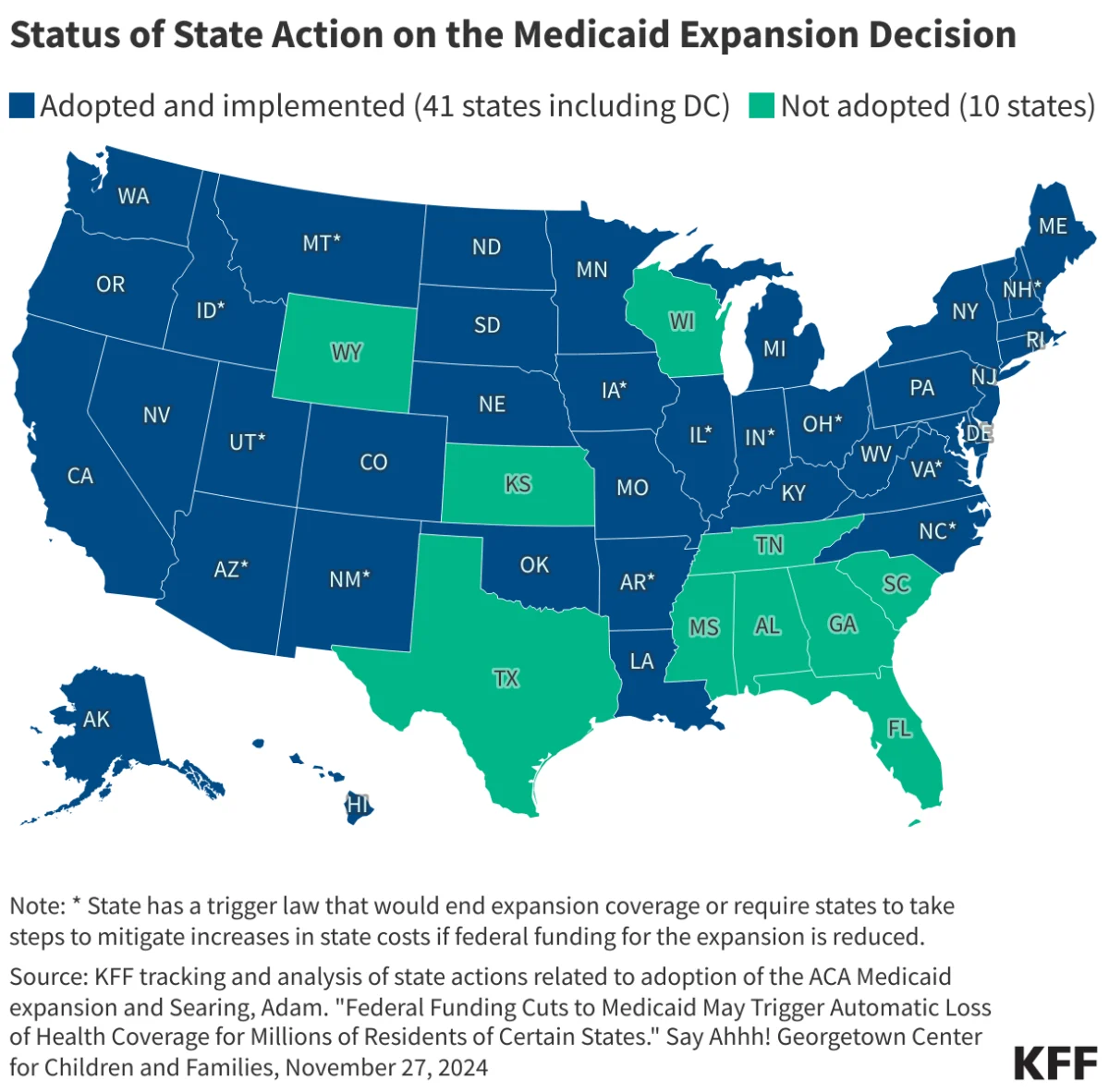
As of the most recent tracking by the Kaiser Family Foundation (KFF), 41 states—including the District of Columbia—have opted to adopt the expansion. Conversely, 10 states continue to hold out, citing concerns over long-term fiscal sustainability, ideological opposition to federal mandates, or philosophical disagreements regarding the role of government in social welfare. This binary divide has created a systemic inequality in health outcomes, where millions of Americans in non-expansion states remain ineligible for Medicaid while earning too little to qualify for subsidized marketplace insurance.
Chronology: A Decade of Policy Evolution
The trajectory of Medicaid expansion has been marked by legislative battles, judicial intervention, and shifting political winds.
The Legislative Birth (2010)
When the Patient Protection and Affordable Care Act was signed into law, the Medicaid expansion was initially drafted as a mandatory requirement for all states. The vision was a universal, nationwide floor for low-income health coverage.
The Judicial Pivot (2012)
The Supreme Court’s landmark ruling in National Federation of Independent Business v. Sebelius fundamentally altered the ACA’s trajectory. While the Court upheld the constitutionality of the individual mandate, it struck down the federal government’s authority to withhold existing Medicaid funding from states that refused to participate in the expansion. By making the expansion optional, the Court transformed a federal mandate into a state-level policy choice, setting the stage for the political polarization that continues to this day.
The Wave of Adoption (2013–2020)
In the years following the ruling, a steady stream of states moved to adopt the expansion. Initial adoption was largely driven by states with Democratic leadership, but the narrative shifted as the economic benefits—such as hospital stability and increased federal revenue—became apparent. Several conservative states, including Arkansas, Kentucky, and Indiana, pioneered unique "waiver" models, incorporating elements like work requirements or premium contributions to align the expansion with more traditional conservative health policies.
The Modern Era (2021–Present)
The American Rescue Plan Act of 2021 introduced a new financial incentive: a temporary, two-year increase in the base FMAP for states that newly expanded. This served as a catalyst for a second wave of adoption, bringing states like Missouri and South Dakota into the fold through voter-led ballot initiatives. Today, the expansion movement is increasingly driven by grassroots efforts rather than legislative action, as voters in red states frequently circumvent skeptical state legislatures to approve expansion at the ballot box.
Supporting Data: The Economic and Health Impact
The empirical data surrounding Medicaid expansion paints a compelling, if complex, picture of its efficacy.
Reducing the Uninsured Rate
Research consistently shows that states that expanded Medicaid have seen a significantly larger decline in their uninsured rates compared to non-expansion states. The "coverage gap"—those with incomes above Medicaid eligibility but below the threshold for premium tax credits—remains the primary source of the uninsured population in non-expansion states.
Hospital and Provider Stability
For rural hospitals, which operate on razor-thin margins, the expansion has acted as a lifeline. By converting charity care (uncompensated care) into reimbursed services, hospitals in expansion states have seen a marked reduction in closures and financial distress. Conversely, non-expansion states continue to see a higher rate of rural hospital closures, exacerbating the "healthcare deserts" that plague rural America.
Fiscal Impacts
Critics often point to the long-term cost to state treasuries. However, independent analyses, including those from the Government Accountability Office (GAO), suggest that the expansion often pays for itself through indirect savings. These include reductions in state spending on mental health, corrections, and uncompensated care programs, as well as the economic stimulus provided by federal dollars flowing into local healthcare economies.
Official Responses and Political Friction
The discourse surrounding Medicaid expansion is bifurcated by two distinct schools of thought.
The Argument for Expansion
Proponents, including healthcare advocacy groups and the American Hospital Association, emphasize the moral imperative of health equity. They argue that access to healthcare is a fundamental human right and that expansion is the most efficient mechanism to improve public health outcomes, specifically in addressing maternal mortality, chronic disease management, and the opioid epidemic.
The Argument Against Expansion
Opponents, often represented by state-level conservative think tanks and fiscal hawks, raise concerns regarding the "crowd-out" effect—where individuals move from private insurance to public programs. Furthermore, there is a persistent concern that federal funding promises are inherently unstable. If federal deficits force a restructuring of the FMAP in the future, state budgets could be left exposed to significant, unforeseen liabilities. Additionally, ideological opposition centers on the belief that Medicaid fosters a culture of government dependency rather than promoting private-market solutions and individual responsibility.
Implications: The Future of the Safety Net
The status of the 10 remaining non-expansion states represents the final frontier of the ACA’s original vision. As these states continue to evaluate their positions, the implications for the American healthcare system are profound.
Health Equity and Demographic Disparities
The data reveals that the lack of expansion disproportionately affects minority populations and low-income workers in the service, agricultural, and hospitality industries. By failing to expand, non-expansion states are essentially choosing to accept a lower standard of baseline health for their most vulnerable citizens.
The Role of Voter Initiatives
As legislative gridlock persists in many state houses, the rise of ballot initiatives—as seen in Oklahoma, Nebraska, and South Dakota—suggests that the public’s appetite for expansion often exceeds that of their elected representatives. This trend may force a confrontation in the remaining states, as the political cost of opposing the expansion begins to outweigh the ideological benefit.
The Path Toward Universal Coverage
Looking forward, the debate is shifting from "if" to "how." Many policymakers are exploring "Medicaid-like" alternatives for non-expansion states—such as state-subsidized marketplace plans—to capture some of the benefits of expansion without technically adopting the Medicaid framework. However, these "work-arounds" often fall short of the comprehensive, low-cost coverage provided by traditional Medicaid.
Conclusion
The Medicaid expansion is more than just a policy; it is a barometer of the American political consensus on health. While 41 states have embraced the federal-state partnership, the 10 holdouts serve as a reminder that the U.S. remains a nation of fractured policy. As the ACA enters its second decade, the focus will likely shift toward reconciling these differences, addressing the fiscal concerns of remaining states, and determining whether the United States will ever achieve a truly uniform standard of care for its low-income citizens. The data is clear: Medicaid expansion saves lives, stabilizes healthcare infrastructure, and improves economic mobility. Whether the remaining states choose to join this movement will define the health of the American public for generations to come.