Main Facts: The Intersection of Vascular Health and Surgical Outcomes
In a significant development for oncology and surgical planning, a comprehensive systematic review and meta-analysis published in the journal Diagnostics (May 2026) has identified a direct correlation between preoperative abdominal vascular health and the risk of complications following colorectal cancer (CRC) surgery.
The study, led by researchers at the "Iuliu Hațieganu" University of Medicine and Pharmacy and the "Octavian Fodor" Regional Institute of Gastroenterology and Hepatology in Cluj-Napoca, Romania, suggests that preoperative CT scans—already a standard part of the diagnostic work-up for CRC—contain hidden data that could serve as powerful prognostic biomarkers. Specifically, the presence of calcification and stenosis in the abdominal vasculature is strongly associated with an increased likelihood of anastomotic leakage (AL)—a life-threatening complication where the surgical join between two sections of the bowel fails to heal properly.
The research team, spearheaded by Mihnea-Ionuț Nicoară and Mihai Adrian Socaciu, concluded that patients exhibiting a high "calcification burden" on their baseline CT scans are three times more likely to experience any form of anastomotic leakage. Furthermore, the risk of severe, grade C leakage—which often necessitates emergency re-intervention—is significantly elevated, underscoring the clinical importance of evaluating vascular integrity before a patient ever enters the operating room.
Chronology of the Research
The journey toward these findings began with a systematic recognition of the limitations in current surgical risk stratification.
- Initial Concept (2025): The research team identified that while traditional risk factors such as age, BMI, and tumor location are routinely assessed, the role of pre-existing subclinical vascular disease remained under-investigated. The protocol for this study was formally registered in PROSPERO (CRD420251248044) in early 2025.
- Data Collection (2025–2026): Utilizing PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, the researchers conducted an exhaustive search across major databases including MEDLINE/PubMed, Embase, Web of Science, and Google Scholar.
- Submission and Peer Review (April–May 2026): The manuscript was submitted on April 4, 2026. Following a rigorous peer-review process, it was revised and accepted within a month, reflecting the urgent interest in optimizing colorectal surgical outcomes.
- Publication (May 9, 2026): The study was published in Diagnostics, Vol. 16, issue 10, providing a new evidence-based framework for preoperative surgical assessment.
Supporting Data: Quantifying the Risk
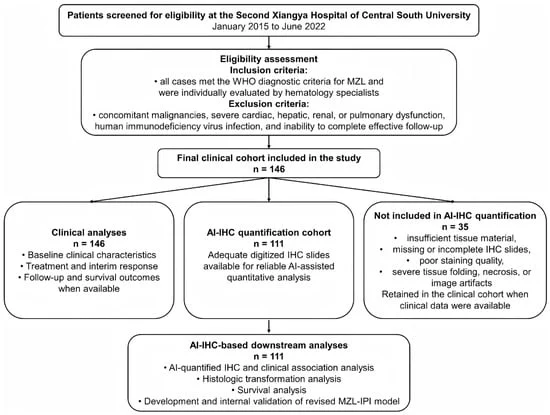
The meta-analysis included 14 distinct studies, comprising a total of 6,712 participants. Quantitative synthesis was performed on 12 of these studies, providing a robust statistical foundation for the conclusions drawn.
Key Statistical Findings:
- Overall Anastomotic Leakage (AL): The pooled analysis showed an Odds Ratio (OR) of 3.08 (95% CI 2.09–4.54) for patients with a higher calcification burden, indicating a three-fold increase in risk compared to those with lower or no detectable calcification.
- Severe (Grade C) AL: For the most critical form of leakage, the OR was 2.68 (95% CI 1.03–6.97). This suggests that vascular health is not just a predictor of minor complications, but a significant factor in the occurrence of major surgical catastrophes.
- Major Morbidity: While the data regarding general major morbidity (OR 1.99) remained slightly imprecise due to the smaller sample size (n=841) within this sub-analysis, the trend strongly points toward an increased risk for patients with compromised vascular health.
The researchers employed random-effects models to ensure that the heterogeneity of the included studies did not skew the findings. Sensitivity analyses were also performed, including a "trim-and-fill" analysis to account for potential publication bias, which confirmed the robustness of the results with an adjusted OR of 2.39.
Clinical Implications and Surgical Strategy
The implications of this research are profound for colorectal surgery units worldwide. Currently, surgeons prioritize tumor staging and anatomy when planning resections. However, this study advocates for the integration of "vascular mapping" into the standard preoperative report.
Standardizing the Preoperative Workflow
The authors emphasize that because CT scans are already being performed to stage the cancer, no additional radiation or financial burden is placed on the patient. The challenge lies in the systematic interpretation of existing images. If radiologists can standardize the reporting of calcification and mesenteric stenosis, surgeons could modify their approach in high-risk patients.
Potential surgical modifications could include:
- Increased Vigilance: Identifying high-risk patients during the preoperative phase allows for more frequent monitoring in the immediate postoperative period.
- Surgical Technique Adjustments: Surgeons might opt for a defunctioning stoma more frequently in patients with evidence of severe vascular disease to protect the anastomosis, even if the primary resection appears straightforward.
- Enhanced Recovery Protocols: Patients identified as high-risk through this diagnostic biomarker could be prioritized for specialized perioperative care to improve tissue perfusion and healing potential.
Official Perspectives and Future Directions
In their discussion, the authors note that while the current evidence is compelling, there is a need for prospective studies to standardize these diagnostic methods. "CT-derived vascular disease markers are associated with higher odds of AL after CRC surgery," the authors stated in their conclusion. "Prospective studies should now focus on testing the clinical utility of these markers in randomized controlled trials."
The Need for Standardization
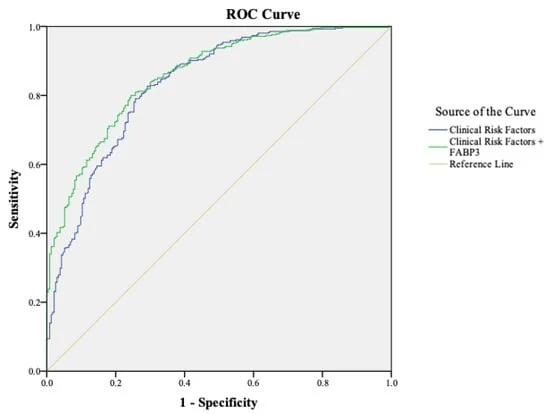
One of the key hurdles identified by the study is the lack of consistency in how "calcification burden" is measured across different centers. The research found that studies using Receiver Operating Characteristic (ROC) cut-points yielded different effect sizes than those using non-ROC methods, highlighting a need for a universal scoring system for abdominal vascular health.
Moving Forward
The research team is calling for the creation of a standardized, automated, or semi-automated software tool that can assist radiologists in quantifying vascular calcification during routine CT reporting. By turning qualitative observations into quantitative, actionable data, hospitals could significantly reduce the incidence of anastomotic leakage, thereby shortening hospital stays, reducing healthcare costs, and, most importantly, improving patient survival and quality of life.
Conclusion
The study by Nicoară et al. represents a paradigm shift in how clinicians view preoperative imaging. By looking beyond the tumor and into the patient’s systemic vascular health, surgeons can better anticipate complications and tailor their approach. As the field of precision medicine continues to expand, the ability to utilize existing diagnostic data to predict individual surgical risks will likely become a cornerstone of high-quality oncological care. This systematic review serves as a vital call to action for the medical community to refine preoperative protocols and embrace the prognostic potential of the abdominal vasculature.
Citation: Nicoară, M.-I.; Socaciu, M.A.; Ursu, D.; Ciocan, A.; Al Hajjar, N. Preoperative CT Evaluation of Abdominal Vasculature and the Risk of Surgical Complications in Colorectal Cancer Resection with Anastomosis: A Systematic Review and Meta-Analysis. Diagnostics 2026, 16, 1449. https://doi.org/10.3390/diagnostics16101449