Since its first description by Edward Stafne in 1942, the Stafne Bone Cavity (SBC)—a distinct, asymptomatic, radiolucent lesion typically found in the posterior region of the mandible—has remained one of the most intriguing puzzles in oral and maxillofacial surgery. While modern diagnostic imaging has made these cavities easier to spot, the fundamental "why" behind their formation has eluded researchers for decades.
A recent pilot study, published in Diagnostics, has broken new ground by applying advanced mathematical modeling to this clinical mystery. By integrating 3D cone-beam computed tomography (CBCT) volumetric data with 2D fractal dimension (FD) analysis, researchers have sought to determine whether the bone quality surrounding these lesions holds the secret to their elusive origins.
The Main Facts: What is a Stafne Bone Cavity?
The Stafne Bone Cavity is a developmental anatomical variation rather than a true neoplasm. Typically located between the mandibular canal and the base of the mandible, it appears as a radiolucent (dark) area on dental radiographs. Despite its often alarming appearance, the condition is benign and asymptomatic, meaning it does not cause pain or physical impairment.

For years, the medical community has debated its etiology. The prevailing theory suggests that the cavity is created by chronic mechanical pressure—often attributed to the submandibular salivary glands or abnormal vascular pulsations of the facial artery—which causes the bone to remodel and thin over time. However, this theory is incomplete: if these anatomical structures are universal in the human population, why does the Stafne Bone Cavity occur in only a small fraction of individuals? This central question drove the recent investigation into the trabecular microarchitecture of the jaw.
Chronology of the Investigation
The study was designed as a retrospective analysis, screening 2,500 CBCT images to identify rare cases of SBC. The timeline of this research follows a rigorous scientific methodology:
- Initial Screening: Researchers scanned 2,500 patient records to isolate 14 confirmed cases of SBC.
- Cohort Formation: A control group of 14 patients, matched by age and gender to ensure statistical parity, was established.
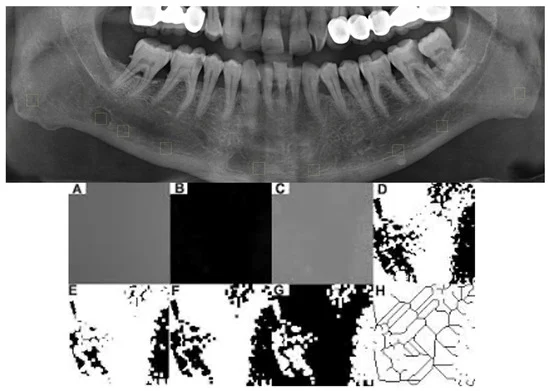
- Data Processing: Using ImageJ software, researchers performed fractal dimension analysis—a mathematical method used to quantify the complexity of trabecular (spongy) bone.
- Volumetric Mapping: CBCT data was processed via ITK-Snap to perform semi-automatic segmentation, allowing for precise 3D measurement of the lesion volumes (in mm³).
- Statistical Validation: A post-hoc power analysis was conducted to determine the reliability of the findings, with the team presenting their preliminary results at the 5th International Congress of the Oral Diagnosis and Maxillofacial Radiology Society.
Supporting Data: Fractal Dimensions and Bone Quality
The core of the study relied on Fractal Dimension (FD) analysis. FD is a robust, non-invasive computational tool that characterizes the "complexity" of bone tissue. If a bone is structurally compromised or has undergone aggressive remodeling, its FD value typically changes.

The findings were revealing:
- Numerical Discrepancies: While FD values within the SBC regions were numerically lower than those in healthy control regions, the difference did not reach statistical significance.
- Structural Preservation: The data suggests that the trabecular microarchitecture remains largely preserved in and around the cavity. This indicates that the SBC does not trigger a radical, aggressive bone-destructive process.
- Volume Correlation: The study measured an average SBC volume of 635.6 ± 460.8 mm³. Interestingly, there was no significant correlation between the size of the cavity and the complexity of the surrounding bone, reinforcing the idea that the lesion is a static, rather than progressive, anatomical entity.
- Reproducibility: Interobserver reliability was excellent, with Intraclass Correlation Coefficients (ICC) ranging between 0.91 and 0.96, proving that the methodology for measuring these tiny, complex structures is highly reliable for future clinical use.
Official Responses and Clinical Implications
The researchers, led by N.G.I. and G.A., conclude that the Stafne Bone Cavity should be categorized as a structural developmental variation rather than an aggressive pathological process. The absence of significant alterations in bone microarchitecture is a critical finding for clinicians.
"The preservation of trabecular complexity supports the view that SBC does not represent an intrinsic pathological process affecting bone microarchitecture," the researchers noted in their discussion. "It may instead reflect an adaptive response to adjacent soft tissue structures."

From a clinical standpoint, this is reassuring. For dentists and oral surgeons who encounter these radiolucencies during routine panoramic radiography or CBCT scans, the study provides evidence that these lesions do not necessarily require aggressive intervention. Instead, the focus should remain on monitoring. Because the bone structure is not "destroyed" in a typical pathological sense, the risk of fracture or secondary disease appears minimal.
Implications for Future Research
While this study offers a significant step forward, the authors are careful to label it "exploratory." The primary limitation—a small sample size—reflects the inherent rarity of the condition. However, the study serves as a "hypothesis-generating" framework that sets the stage for larger, multicenter studies.
Key Takeaways for the Medical Community:
- Standardization: The use of FD analysis as a quantitative measure for jawbone quality has been validated by this study, providing a template for future bone health assessments.
- Etiological Shift: The research leans away from the "pressure-induced damage" theory and toward a more static "developmental variation" model.
- Diagnostic Confidence: Clinicians can use these findings to support a more conservative approach to patient management, avoiding unnecessary surgical biopsies for confirmed, asymptomatic SBCs.
The study also underscores the technological challenges in the field. While CBCT is the gold standard for viewing the 3D structure of the jaw, its voxel size can sometimes obscure fine trabecular detail. The team’s decision to integrate 2D fractal analysis into their 3D volumetric study highlights a "best-of-both-worlds" approach that navigates the current technological limitations of dental imaging.

Conclusion: A Piece of the Puzzle
The "Stafne Enigma" remains partially unsolved, but the shroud of mystery is thinning. By moving beyond subjective visual interpretation and into the realm of mathematical quantification, researchers have confirmed that the Stafne Bone Cavity is a quiet, stable neighbor within the human mandible. As medical imaging technology continues to evolve, future studies utilizing high-resolution AI-assisted segmentation and longitudinal data will likely confirm that these cavities are not signs of pathology, but simply unique fingerprints of human anatomical development.
For now, the message to the dental community is clear: observe with confidence, analyze with precision, and avoid the assumption that every radiolucency requires a surgical cure. The bone, as this study suggests, is perfectly capable of adapting to its environment without losing its structural integrity.