By Editorial Staff
July 14, 2026
The promise of artificial intelligence in healthcare has long been framed as a clinical revolution: algorithms detecting cancers earlier, personalized medicine tailoring drug regimens, and predictive analytics preventing hospital readmissions. However, as AI integration accelerates, a parallel, more contentious battle is playing out behind the scenes. In the back offices of hospitals and the claims departments of insurance companies, a "quiet arms race" is currently unfolding, threatening to redefine the financial landscape of the U.S. health system.
In the latest episode of the podcast series The Business of Health, host Chip Kahn sat down with Caroline Pearson, Executive Director of the Peterson Health Technology Institute (PHTI), to dissect the reality of AI adoption. The conversation highlights a sobering question: Is this technological surge actually lowering the cost of care, or is it merely accelerating a high-stakes tug-of-war over the American healthcare dollar?
The Core Conflict: Automation vs. Escalation
As providers deploy sophisticated AI tools to automate medical coding, billing, and revenue capture, insurers are deploying counter-algorithms designed to review, deny, and hold the line on expenditures. This cycle of technological escalation creates a paradox where efficiency gains may be entirely offset by the administrative burden of the "fight."
"We are seeing a massive investment in tools that fundamentally do not change the delivery of care," Pearson noted during the episode. "Instead, they change the speed and intensity of the billing and authorization process."
The primary concern, according to Pearson, is that the current incentive structure encourages players to use AI as a weapon for margin protection rather than a tool for clinical improvement. If hospitals use AI to maximize their billing codes while insurers use it to trigger automated claim denials, the net result for the patient is often increased friction, not reduced costs.
A Chronology of the AI Administrative Shift
To understand how we arrived at this impasse, it is necessary to look at the timeline of digital health adoption over the past half-decade:

- 2021–2022: The Initial Hype Cycle. Early adoption of AI was focused on basic electronic health record (EHR) scribing and simple, rule-based automation. The narrative was overwhelmingly positive, centered on reducing "physician burnout."
- 2023: The Proliferation of Digital Tools. The market saw a surge in digital diabetes tools and chronic condition management apps. This period was marked by massive venture capital investment, promising that tech-enabled monitoring would "lower the total cost of care."
- 2024: The Reality Check. Independent assessments, notably those led by the Peterson Health Technology Institute, began to surface data showing that many of these digital tools were not, in fact, reducing total healthcare spending. The "famous assessment" of digital diabetes tools became a watershed moment, proving that engagement does not always equate to cost-savings.
- 2025: The Arms Race Escalates. As providers and payers realized that AI could be used to optimize revenue cycles and streamline denials, the focus shifted from patient health outcomes to administrative throughput.
- Mid-2026: The Current State. We are now in a period where prior authorization and medical billing have become the primary battlegrounds for AI implementation. The focus has shifted toward regulatory scrutiny and the demand for rigorous, evidence-based evaluations of health tech.
Supporting Data: The Efficiency Gap
The Peterson Health Technology Institute (PHTI) occupies a unique vantage point in this landscape. By running rigorous, independent evaluations, the institute provides the evidence that stakeholders often prefer to ignore.
A recurring theme in PHTI’s research is the disconnect between "activity" and "value." In many of the technologies analyzed by Pearson’s team, the systems successfully increased the number of administrative transactions performed per hour. However, when those transactions were audited against clinical outcomes, the impact on total cost of care was frequently negligible or, in some cases, additive.
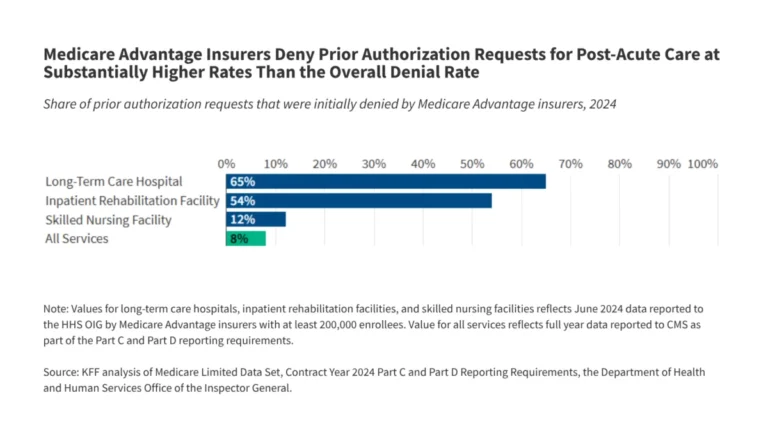
For example, when evaluating prior authorization—a process historically fraught with manual delays—AI proponents argued that automation would speed up approvals. In practice, the data suggests that while the speed of the initial review increased, the complexity of the appeals process often expanded, creating a new, AI-driven administrative layer that consumes time and resources without necessarily improving patient access to care.
The Role of Incentives and Policy
"Whether AI delivers better care or just more activity depends entirely on how we align incentives," Pearson argued. Currently, the U.S. fee-for-service model provides little reward for efficiency. If a hospital can use AI to squeeze an extra 3% in revenue from a claim, they have every incentive to do so. Conversely, if an insurer can use AI to automate the denial of high-cost services, they protect their bottom line.
Regulatory Perspectives
Policy experts and oversight bodies, including those aligned with the Peterson Center on Healthcare, are beginning to call for:
- Transparency Requirements: Mandating that AI models used in decision-making be auditable for bias and efficacy.
- Outcome-Based Reimbursement: Moving away from paying for the "transaction" (the billing event) and toward paying for the "outcome" (the patient’s health status).
- Standardization of Prior Authorization: Creating industry-wide protocols for AI-driven reviews to prevent the "black box" denials that currently plague the system.
Without these guardrails, the technology risks becoming an engine for cost-inflation rather than cost-containment.
Implications: The Future of the Health System
The implications of this administrative arms race are profound for both the industry and the patient.

For Providers and Payers
The current trajectory suggests that the "administrative burden" will not disappear; it will merely evolve into a digital one. Hospitals that fail to invest in these revenue-cycle AI tools risk financial insolvency, while insurers that fall behind in their defensive AI capabilities risk overpaying for services. This creates a "mandatory" investment environment that diverts capital away from clinical innovation, such as upgrading diagnostic equipment or improving frontline nursing ratios.
For the Patient
The patient remains the silent bystander in this technological war. For the average consumer, the experience of healthcare remains fragmented. If AI is used primarily to argue over payments, the patient faces the same hurdles—denied coverage, complex billing statements, and delays in care—just at a faster, algorithmically determined pace.
Conclusion: Bridging the Gap
As Chip Kahn noted in the conclusion of the episode, the objective of the healthcare system should be to deliver "better care at lower cost." Currently, the administrative AI arms race is failing that mission.
Caroline Pearson’s work at the Peterson Health Technology Institute remains a critical check on the industry. By demanding rigorous evidence, PHTI is pushing the sector to move past the "shiny object" phase of AI adoption. The hope for the future lies in shifting the focus from using AI to fight over the existing healthcare dollar to using AI to actually optimize the clinical journey.
As we look ahead, the regulatory landscape will be the defining factor. Will policy-makers intervene to ensure AI serves the patient, or will the "arms race" continue to prioritize the ledger over the patient? The answer to that question will determine whether the next decade of healthcare technology is a success story or a missed opportunity.
About the Host: Charles N. Kahn III is a senior visiting fellow at KFF, a visiting senior fellow at the American Enterprise Institute, and a nonresident senior scholar at the University of Southern California’s Schaeffer Center for Health Policy & Economics. He is a prominent voice in the discourse on healthcare economics and policy.
About the Guest: Caroline Pearson is the Executive Director of the Peterson Health Technology Institute (PHTI) and the Peterson Center on Healthcare. Her extensive background includes leadership roles at NORC at the University of Chicago and Avalere Health, with a career dedicated to creating a high-performing, cost-effective health system.