Since its inception, the Patient Protection and Affordable Care Act (ACA) has served as the bedrock of modern American health policy. At the heart of this legislative framework lies the Medicaid expansion—a transformative provision designed to close the coverage gap for millions of low-income Americans. As we move further into the 2020s, the national map of healthcare access remains starkly divided, reflecting deep-seated ideological, economic, and political disparities between states.
The Foundation: Understanding the Medicaid Expansion
The Affordable Care Act’s Medicaid expansion was designed to be a paradigm shift in how the United States approaches the social safety net. Prior to the ACA, Medicaid was primarily restricted to specific categories of low-income individuals: children, pregnant women, the elderly, and those with disabilities. The ACA fundamentally altered this eligibility structure by decoupling coverage from categorical status and linking it instead to financial need.
Under the provisions of the law, Medicaid eligibility was expanded to nearly all adults with household incomes up to 138% of the Federal Poverty Level (FPL). In 2025, for an individual, this threshold translates to an annual income of $21,597. This change was intended to reach the "working poor"—individuals who earn too much to qualify for traditional Medicaid but too little to afford private health insurance on the open market.
To encourage states to participate, the federal government provided a robust financial incentive: an enhanced Federal Medical Assistance Percentage (FMAP). For the expansion population, the federal government covers 90% of the costs, significantly easing the fiscal burden on state budgets. Despite this, the Supreme Court’s 2012 ruling in NFIB v. Sebelius rendered the expansion optional, effectively creating the current landscape of fragmented coverage.
Chronology: A Decade of Policy Evolution
The journey of Medicaid expansion has been marked by legislative battles, judicial intervention, and shifting public opinion.
- 2010: The ACA is signed into law by President Barack Obama, mandating a national Medicaid expansion.
- 2012: The Supreme Court rules in NFIB v. Sebelius that the federal government cannot withhold existing Medicaid funding from states that refuse to expand, effectively making expansion a state-level choice.
- 2014: The first wave of states implements the expansion, triggering a surge in enrollment and a significant reduction in the national uninsured rate.
- 2016–2019: A period of "ballot initiative activism." States like Maine, Idaho, Nebraska, and Utah utilize the direct democracy process to bypass reluctant state legislatures and mandate expansion.
- 2020–2024: The COVID-19 pandemic underscores the critical importance of health coverage, leading to further adoptions, including states previously thought to be staunchly opposed, such as Oklahoma and Missouri.
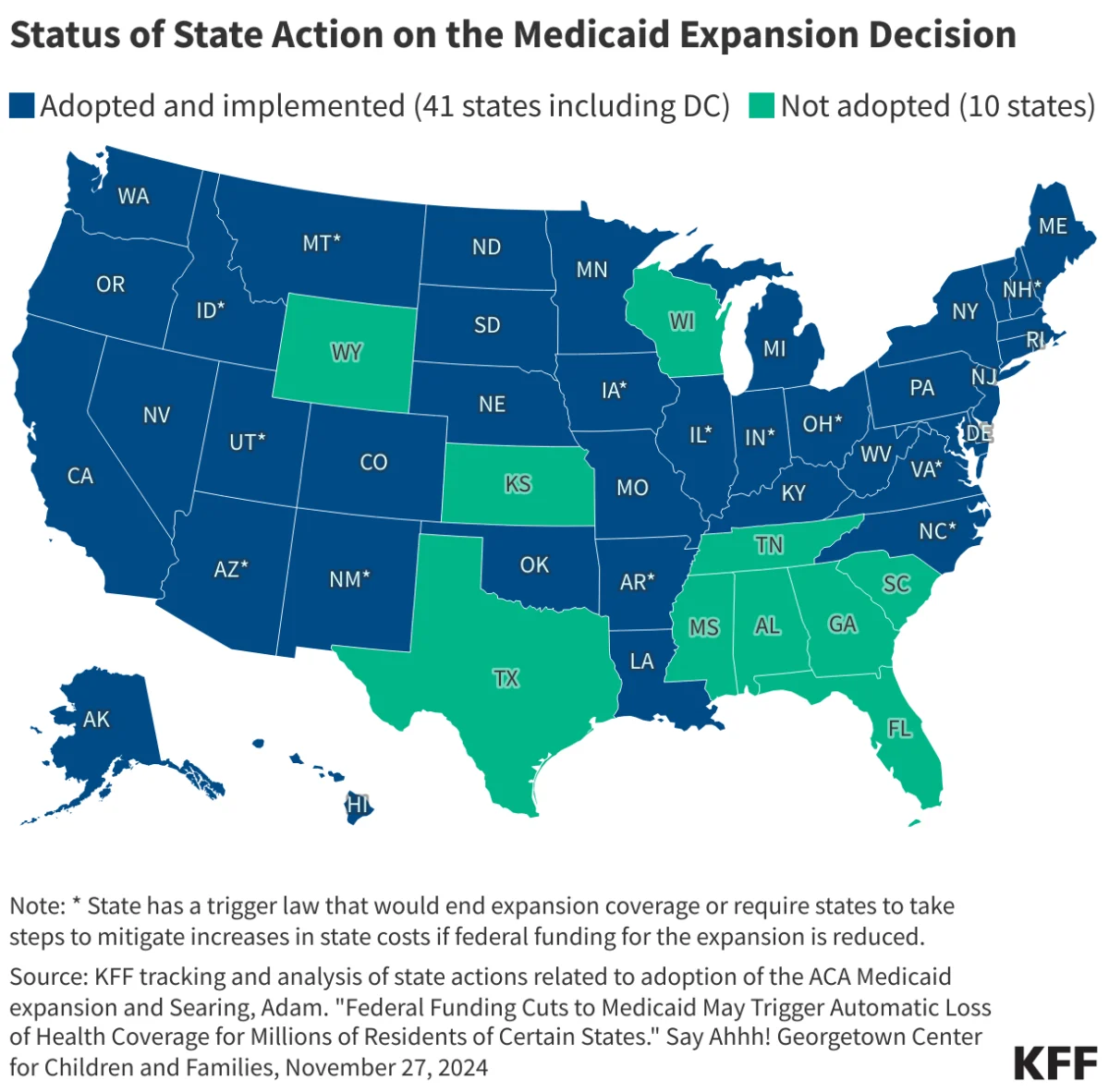
- 2025: The current landscape shows 41 jurisdictions (including the District of Columbia) have embraced the expansion, while 10 states continue to hold out.
The Current Map: A Divided Nation
As of early 2025, the map of Medicaid expansion represents a clear geographic and political divide. KFF (Kaiser Family Foundation) data indicates that 41 states have adopted the policy. These states have successfully integrated millions of new enrollees into the Medicaid system, providing a safety net that has proven vital during economic downturns and public health emergencies.
Conversely, 10 states—primarily clustered in the South and the Midwest—have chosen not to adopt the expansion. In these states, a "coverage gap" persists. Individuals in these regions often earn too much for traditional Medicaid but not enough to qualify for federal subsidies under the ACA marketplace, leaving them in a precarious position regarding access to primary care, preventative screenings, and emergency medical services.
Supporting Data: Economic and Health Outcomes
The data surrounding Medicaid expansion is robust, consistently demonstrating positive outcomes for both state economies and individual health metrics.
Health Access and Quality of Care
Numerous studies have shown that expansion states experience a significant increase in the use of preventative care services. Without the financial barrier of co-pays and deductibles associated with private plans, individuals in expansion states are more likely to manage chronic conditions—such as diabetes and hypertension—before they escalate into expensive, life-threatening emergencies.
The Fiscal Impact
Critics of the expansion often point to the long-term cost to taxpayers. However, proponents highlight the "offset effect." States that expand Medicaid often see a reduction in uncompensated care costs at hospitals. When uninsured patients visit emergency rooms, the costs are often passed on to the public through higher insurance premiums or state-funded safety-net programs. By moving these individuals onto Medicaid, states stabilize their hospital systems and generate significant economic activity through the influx of federal dollars.
Federal Matching Funds (FMAP)
The 90% federal matching rate remains one of the most generous fiscal policies in the history of U.S. social programs. States that have resisted expansion effectively leave billions of federal tax dollars on the table, which are instead redistributed to other states that have chosen to participate.
Official Responses and Political Rhetoric
The debate over Medicaid expansion remains a focal point in state capitols.
Proponents of Expansion argue from a perspective of human rights and economic efficiency. Governors and legislators in expansion states frequently cite the reduction in hospital closures—particularly in rural areas—as the primary justification for their support. They argue that a healthy workforce is a productive workforce and that the federal match is an essential tool for fiscal solvency.
Opponents of Expansion often frame their resistance in terms of "fiscal conservatism" and "limited government." Many state officials in the 10 remaining non-expansion states express concern regarding the sustainability of the federal match, fearing that if the federal government were to lower the FMAP in the future, the state would be left with an unmanageable budgetary hole. Additionally, there is a recurring ideological argument that Medicaid expansion promotes dependence on the state rather than encouraging individuals to seek private employment-based insurance.
Implications: The Road Ahead
The future of the Medicaid expansion is tied to both the federal legislative agenda and state-level political shifts. Several key implications emerge from the current status quo:
1. The Persistence of the Coverage Gap
The existence of the coverage gap remains a major policy failure in the eyes of public health experts. As long as these 10 states remain outside the expansion, a significant portion of the American population will continue to live without a reliable safety net, leading to disparities in life expectancy and health outcomes compared to their peers in expansion states.
2. The Potential for Future Adoptions
The "ballot initiative" model has proven effective in bypassing legislative gridlock. It is highly probable that in the coming years, advocacy groups in the remaining 10 states will continue to pressure state governments, potentially forcing the issue onto future election ballots.
3. Integration with Telehealth and Digital Health
As healthcare systems evolve, the Medicaid population in expansion states is increasingly benefiting from the integration of telehealth. This digital transformation allows for broader access in rural areas where specialist care is scarce, demonstrating that the expansion is not merely about insurance cards, but about modernizing the delivery of medicine.
4. The Federal-State Tension
The tension between state autonomy and federal oversight is unlikely to dissipate. The debate over the "proper" role of government in healthcare continues to be the defining characteristic of American social policy. The Medicaid expansion serves as the primary battleground for these differing visions of the American dream.
Conclusion
The Medicaid expansion is more than just a policy adjustment; it is a fundamental reflection of how a nation values the health of its citizens. While the progress made since 2014 is undeniable—with 41 states having secured coverage for millions of residents—the work remains unfinished. As the data shows, the disparities between states are not merely statistical; they are lived realities for the millions of Americans still waiting for access to affordable, comprehensive healthcare.
Whether the remaining 10 states eventually join the expansion will likely depend on the persistent efforts of policy advocates, the changing political demographics within those states, and the evolving economic evidence that continues to show that expansion is not just a moral imperative, but a sound fiscal strategy. The journey of the ACA continues, and the Medicaid expansion remains its most powerful, yet incomplete, chapter.