Editorial Note: Originally published in November 2009, this resource provides an ongoing, comprehensive analysis of the evolution of U.S. global health policy, specifically concerning the President’s Emergency Plan for AIDS Relief (PEPFAR). This edition reflects data and geopolitical shifts as of early 2025.
Executive Summary: A Turning Point in Global Health
The global HIV/AIDS epidemic remains one of the most formidable challenges to public health and international development in modern history. With approximately 40.8 million people currently living with HIV and a staggering death toll reaching into the tens of millions since the epidemic’s inception, the stakes for international intervention have never been higher. At the heart of this response is the President’s Emergency Plan for AIDS Relief (PEPFAR). Created in 2003, PEPFAR stands as the largest commitment by any nation to address a single disease in history. However, as the program enters its third decade, it faces an unprecedented period of transition, marked by political volatility, shifting administrative priorities, and a fundamental restructuring of how the United States engages with global health partners.
The Global Situation: A Lingering Crisis
Despite decades of progress, the HIV/AIDS epidemic is far from over. While the rapid scaling of antiretroviral therapy (ART) has transformed HIV from a death sentence into a manageable chronic condition for millions, the pace of new infections remains a concern. The global landscape is characterized by deep health inequities, where access to life-saving medication, testing, and preventative tools like pre-exposure prophylaxis (PrEP) is often dictated by geography and socio-economic status.
Current data from 2024 underscores that while the global community has made significant strides, the "last mile" of the epidemic is the most difficult. The intersection of emerging global conflicts, climate-related displacement, and the rise of other health crises has strained the infrastructure built to manage HIV, threatening to reverse years of hard-won progress.
Chronology of the U.S. Response: From Leadership to Uncertainty
The U.S. government’s involvement in the HIV/AIDS crisis began in the mid-1980s, but it was not until the 2003 State of the Union address that President George W. Bush galvanized a new era of global action.
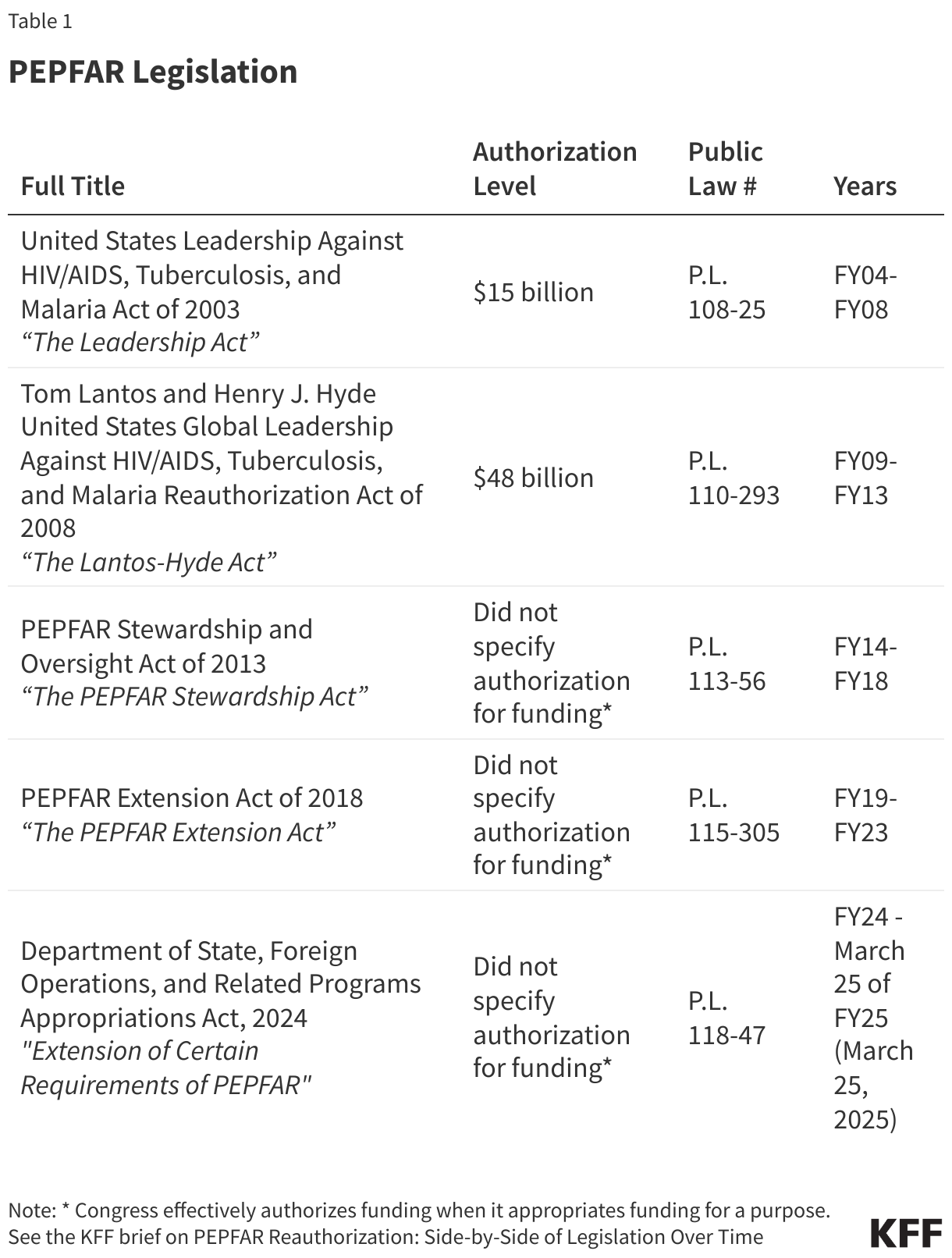
- 2003: The enactment of the Leadership Act officially launched PEPFAR, establishing a robust, multi-billion-dollar framework for bilateral aid.
- 2008: The Lantos-Hyde Act reauthorized the program, reinforcing the U.S. commitment to the Global Fund and expanding the scope of services.
- 2013 & 2018: Subsequent extensions signaled strong, bipartisan support that held firm across multiple presidential administrations.
- 2024: The landscape shifted dramatically. A short-term reauthorization in early 2024, followed by the subsequent lapse of key provisions, marked a departure from the historical consensus. The program became entangled in domestic political debates, specifically regarding abortion and broader foreign aid strategies, creating a "wait-and-see" environment that has hindered long-term planning.
Organizational Evolution: The Rise and Transformation of OGAC
PEPFAR was designed to consolidate U.S. efforts, bringing together the expertise of the Department of State, USAID, the CDC, and other federal agencies under the leadership of the Office of the Global AIDS Coordinator (OGAC).
The Global AIDS Coordinator, holding the rank of Ambassador, has historically served as the linchpin of this effort. However, the current organizational structure is undergoing a profound metamorphosis. Under the second Trump administration, the focus has shifted toward the Bureau of Global Health Security and Diplomacy (GHSD). The integration of HIV activities into broader, more diffuse health security mandates—coupled with significant staff reductions at key agencies like USAID and the CDC—has signaled a shift away from the "siloed" expertise that originally made PEPFAR so effective. Today, the absence of a confirmed Coordinator leaves a leadership vacuum that complicates the transition of services to host-country governments.
Supporting Data: By the Numbers
The statistical impact of PEPFAR is immense, yet recent reports reflect a concerning cooling of momentum.
- Cumulative Lives Saved: Estimates suggest over 26 million lives saved through interventions ranging from ART provision to the prevention of mother-to-child transmission.
- FY 2024 Results: The program supported 83.8 million people with testing services, ensured 20.6 million people were on life-saving antiretroviral therapy, and provided essential care for 6.6 million orphans and vulnerable children.
- The 2025 Trend: Data analysis from Quarter 4 of FY 2025 shows a significant decline in new enrollments for antiretroviral therapy and a drop in PrEP uptake. While the number of individuals already on therapy remains stable, the pipeline of new patients is slowing, indicating potential gaps in outreach and service delivery.
Official Responses and Strategic Shifts
The second Trump administration has fundamentally altered the operational philosophy of PEPFAR. The "America First" Global Health Strategy emphasizes "bilateral global health agreements" over traditional PEPFAR-specific frameworks.
These new agreements require partner nations to take on increasing financial responsibility, effectively offloading the costs of HIV programs from the U.S. taxpayer to host-country governments. While this aligns with the goal of long-term sustainability, critics argue that the pace of this transition—without sufficient time for infrastructure development in developing nations—risks a collapse in quality of care.
Implications: The Future of Global Health Diplomacy
The shift from the established "Country Operational Plan" (COP) model to a broader, less HIV-specific bilateral agreement model has far-reaching implications:
- Diminished Oversight: By removing the specific, granular review processes that defined the original PEPFAR, there is a risk of losing the accountability mechanisms that ensured funds were reaching those most in need.
- Multilateral Relations: The U.S. remains the largest donor to the Global Fund, providing nearly $33 billion since 2001. However, the internal debates over the 33% cap on contributions and the ideological positioning of U.S. aid threaten the stability of the Global Fund’s operations.
- Human Rights and Access: Initiatives like DREAMS, which targeted the vulnerabilities of adolescent girls and young women, have been discontinued. The removal of such specialized programs suggests a move toward a more clinical, less socio-political approach to disease management, which may ignore the root causes of HIV transmission in marginalized populations.
Conclusion: A Legacy at Risk
PEPFAR has been, by any measure, a triumph of American foreign policy and humanitarian commitment. It demonstrated that a concentrated, well-funded, and technically rigorous approach could defeat a pandemic. However, the program currently exists in a state of suspended animation. The transition from a disease-specific powerhouse to a decentralized, co-investment model is a high-stakes gamble.
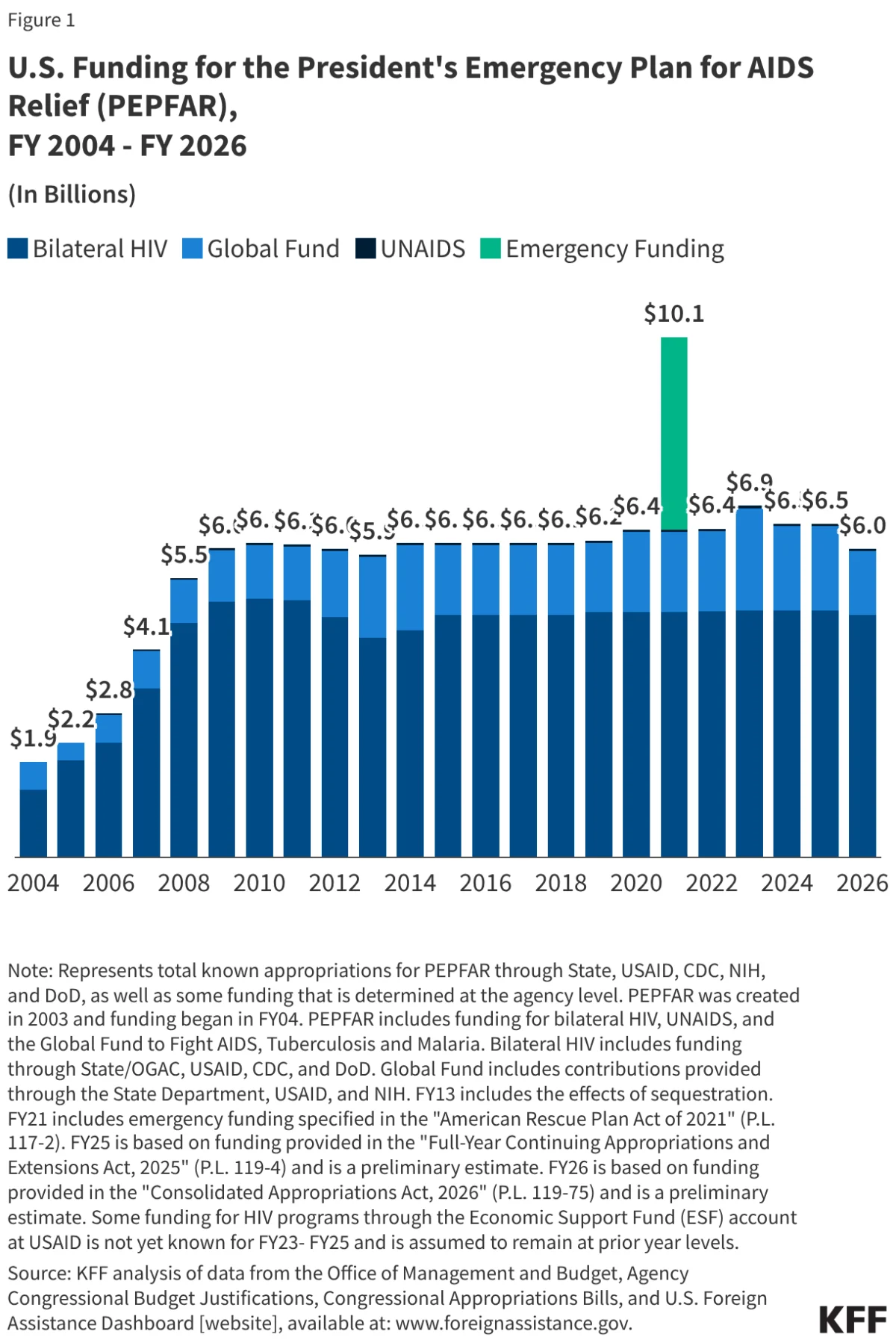
As the U.S. moves toward 2026, the question is not merely one of funding levels—which remain substantial at $6 billion—but of vision. If the infrastructure, expertise, and focus that defined the first two decades of PEPFAR are dismantled, the world may find itself back where it started: fighting a preventable, manageable, but deadly virus without a unified, global strategy. The path forward requires a delicate balance between fiscal responsibility and the moral imperative of global health security. Whether the U.S. can maintain its role as the global leader in the fight against AIDS remains the defining question of the next decade.
For more information on the evolving landscape of global health, refer to the KFF trackers on bilateral health agreements and the legislative history of PEPFAR.