As the United States grapples with a rapidly aging population, the demand for long-term care (LTC) services has reached an unprecedented scale. From home health aides helping the elderly manage daily tasks to nursing assistants providing round-the-clock care in facilities, direct care workers serve as the essential, often invisible, foundation of the American healthcare system. However, a new analysis of 2024 American Community Survey (ACS) data reveals a workforce in crisis—characterized by low wages, high turnover, and an heavy reliance on immigrant labor that is currently facing significant federal policy headwinds.
The Scope of the Challenge: Who Needs Care?
Long-term care is far more than a niche medical service; it is a fundamental societal need. It encompasses a broad range of medical and personal support—from assisting with "activities of daily living" (ADLs) like bathing and eating, to managing complex medication regimens. According to the Department of Health and Human Services (HHS), the reality of aging is stark: more than half of all individuals over the age of 65 will require help with at least two ADLs at some point in their lives.
Crucially, the need for these services is not limited to the elderly. People under 65 living with disabilities also rely heavily on direct care workers to maintain their independence. Medicaid remains the primary payer for these services, and KFF analysis underscores a surprising demographic reality: over half of all individuals utilizing Medicaid-funded long-term care are under the age of 65. Despite this massive demand, the workforce tasked with this care is increasingly fragile.
Chronology of a Growing Crisis
For decades, the direct care sector has struggled with structural instability. The trajectory of this crisis can be mapped through several key developments:
- Early 2000s–2010s: The rise of home-based care models began to shift the labor landscape, moving workers from institutional nursing homes into private homes. While this improved quality of life for patients, it fragmented the workforce and complicated wage and benefit standardization.
- The COVID-19 Pandemic: The pandemic acted as a massive accelerant for existing vulnerabilities. High-stress conditions, coupled with inadequate personal protective equipment and low pay, led to a mass exodus of experienced staff.
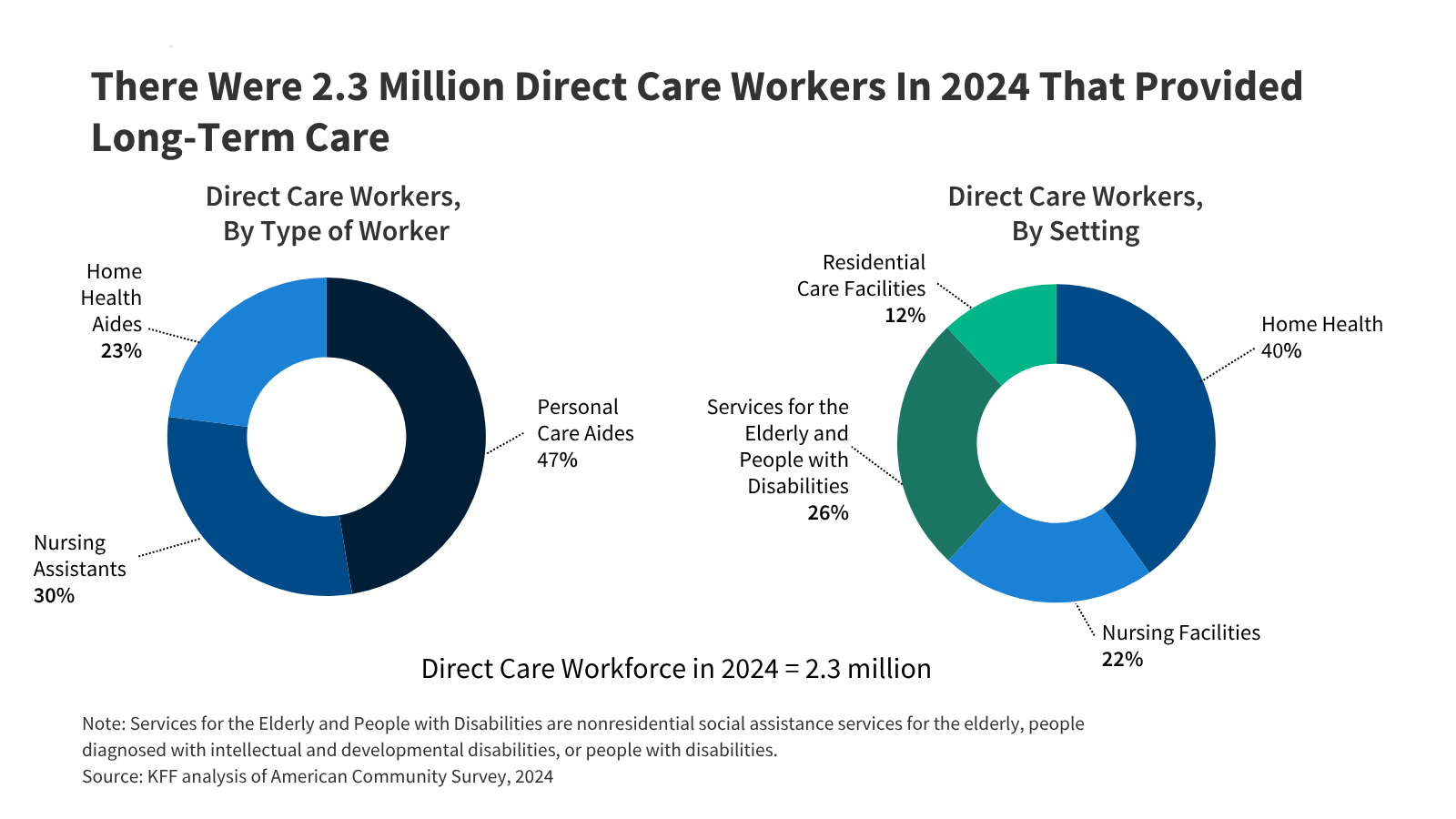
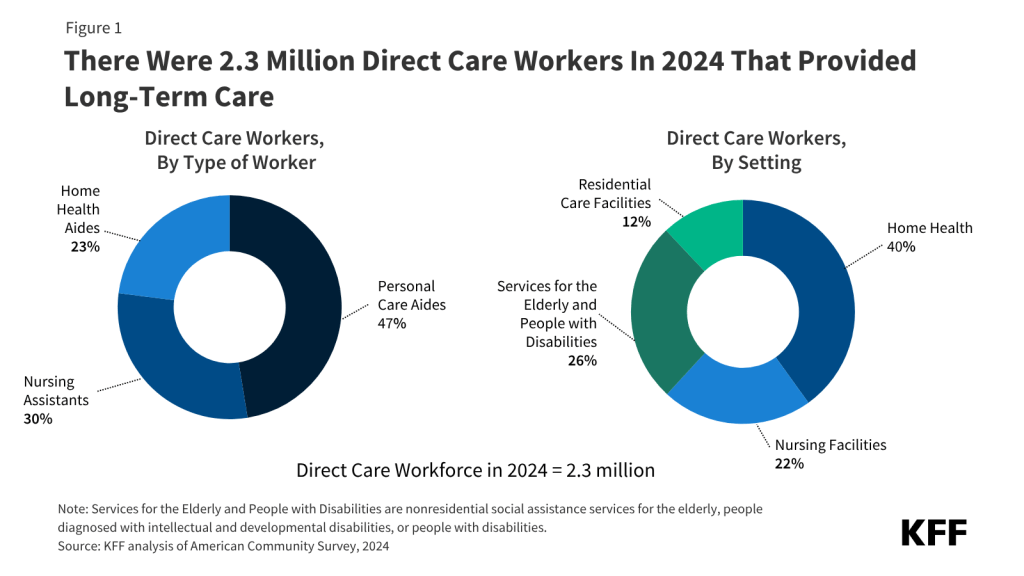
- 2024–2025: The release of the 2024 ACS data in late 2025 confirmed that the workforce had stabilized at approximately 2.3 million workers, but with persistent demographic disparities that make the sector uniquely vulnerable to political and economic shifts.
- 2026 and Beyond: Recent federal policy changes—including stricter visa regulations and the termination of certain Temporary Protected Status (TPS) designations—have introduced new uncertainty for the nearly one-third of the workforce comprised of immigrants.
Supporting Data: A Demographic Snapshot
The 2024 ACS data provides a clear picture of who is providing care in America. The workforce is distinct from the general labor market in several critical ways:
Socioeconomic Vulnerabilities
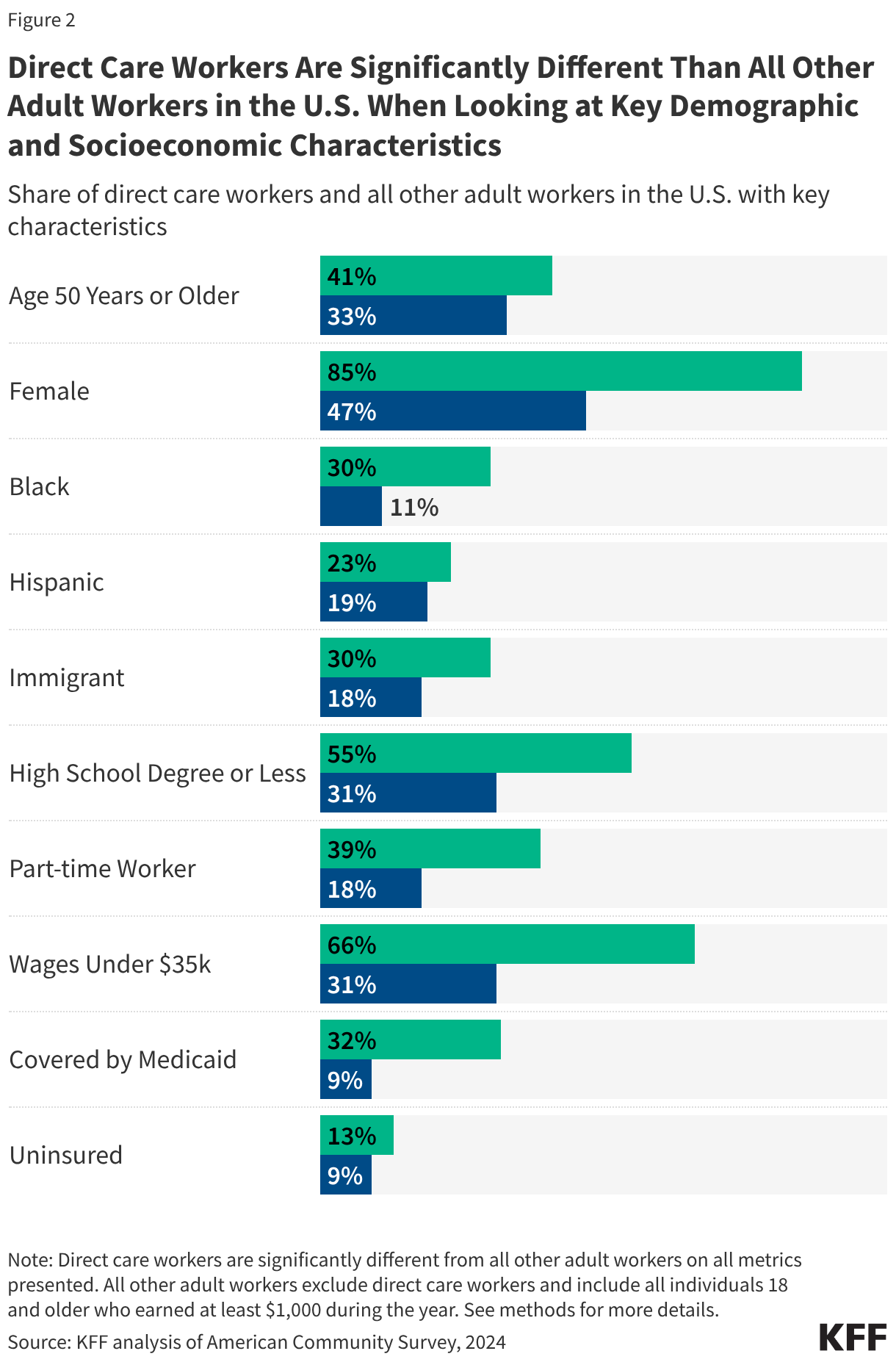
Compared to the average American adult worker, direct care workers are significantly more likely to live on the economic margins. They are:
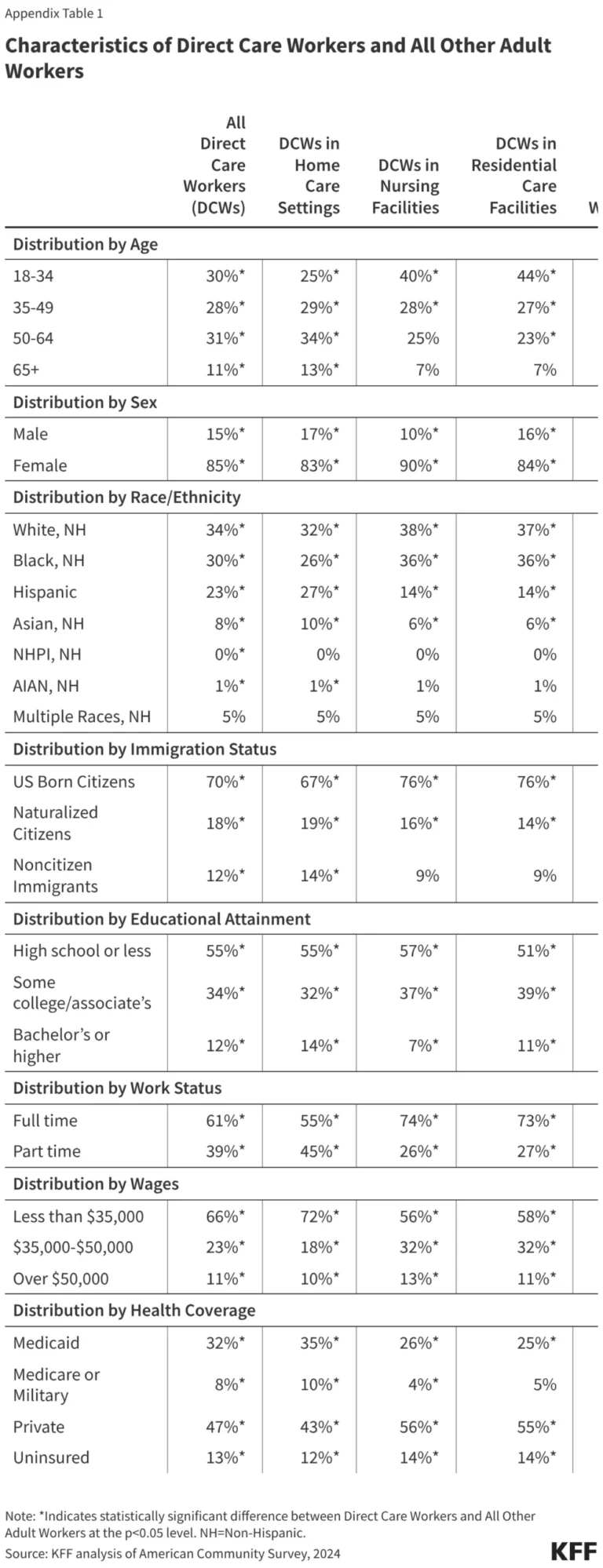
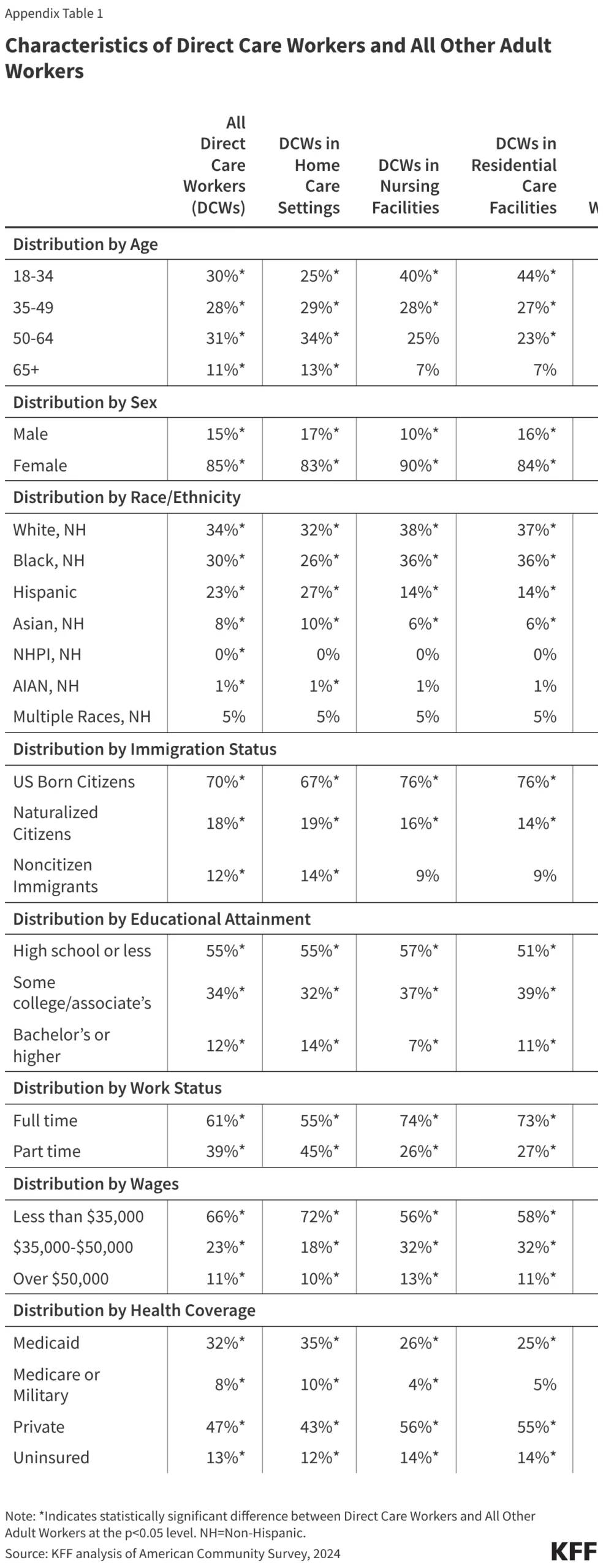
- Less Educated: 55% have a high school diploma or less, compared to 31% of the general workforce.
- Low-Wage Earners: 66% earn less than $35,000 annually, a statistic that correlates with their high reliance on social safety nets. 32% of direct care workers rely on Medicaid for their own health insurance, and 13% remain uninsured.
- Part-Time Reliance: 39% of these workers are employed part-time, which often precludes them from accessing employer-sponsored benefits.
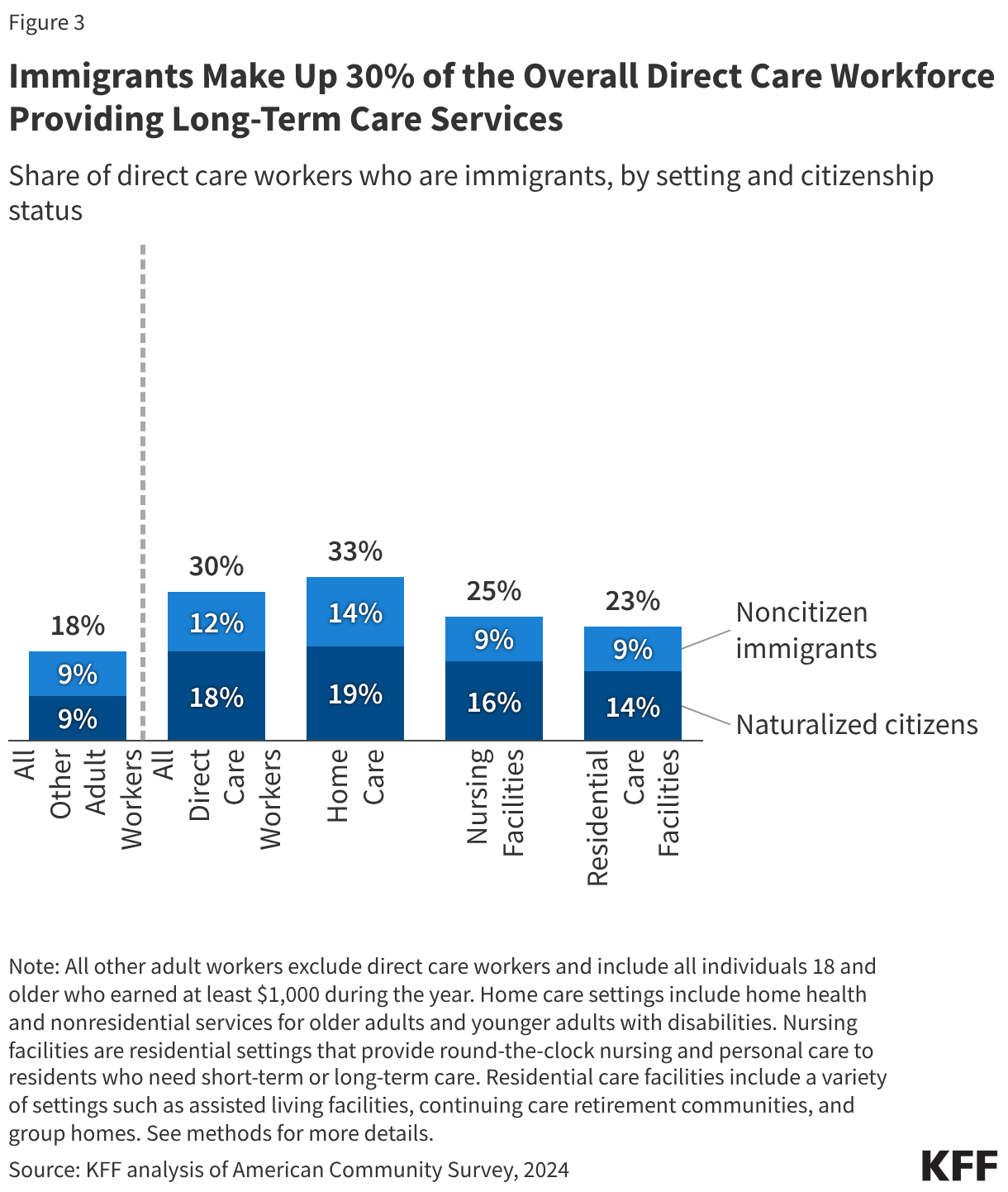
The Role of Immigrant Labor
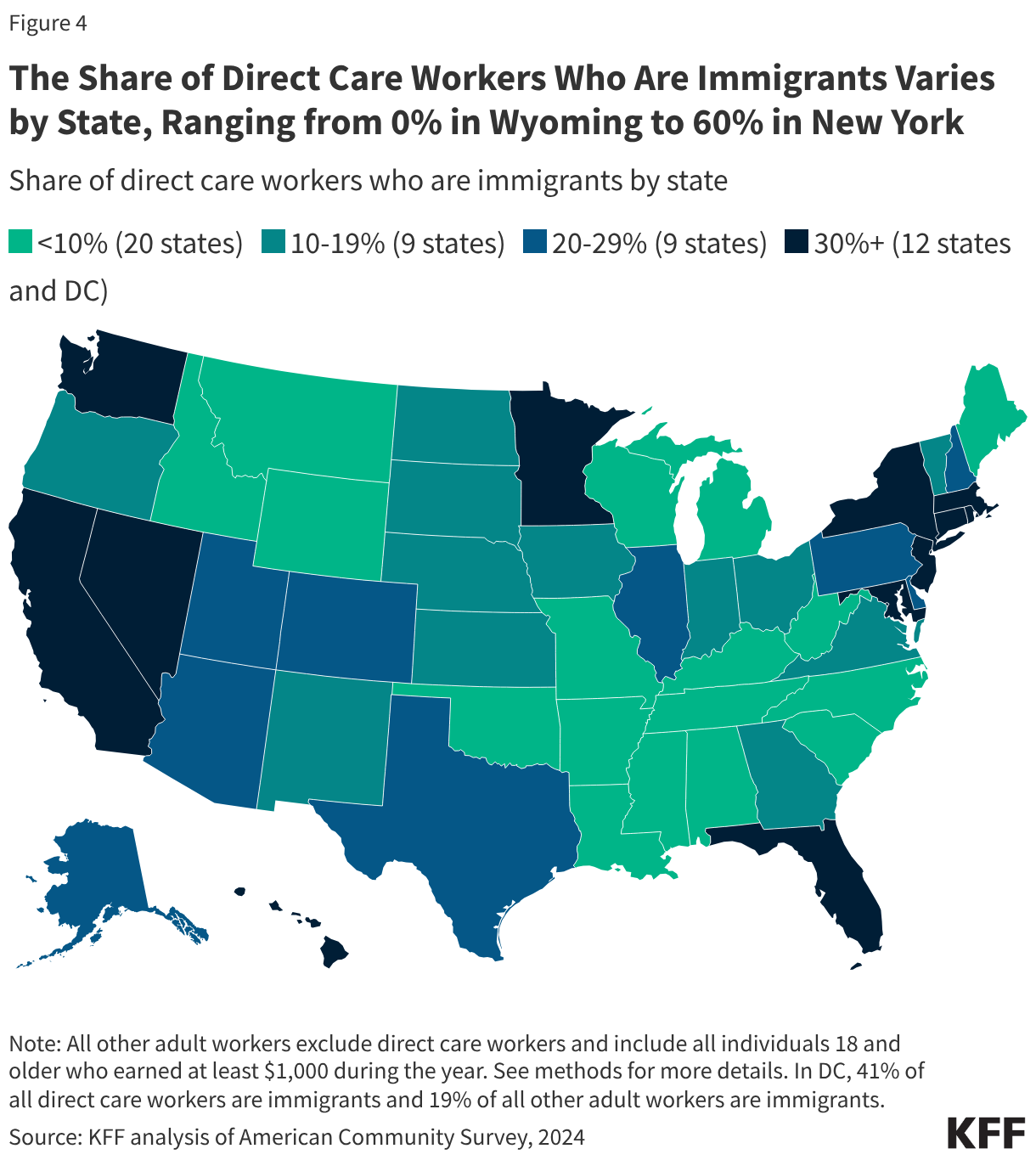
Perhaps the most striking finding is the reliance on immigrant workers. Immigrants make up 30% of the overall direct care workforce—a figure that climbs even higher in home care settings (33%). In some states, such as New York, this reliance is even more pronounced, with immigrants accounting for up to 60% of the care workforce.
These workers are not a monolith; they hail from a diverse array of nations, with nearly two-thirds of immigrant direct care workers originating from just 13 countries. Mexico, the Philippines, Haiti, Jamaica, and the Dominican Republic are among the primary sources of labor. This creates a direct link between national immigration policy and the availability of care for the elderly.
Official Responses and Policy Implications
The intersection of immigration policy and healthcare workforce stability has become a flashpoint for federal authorities. Recent actions by the Trump administration, including the implementation of an immigrant visa pause affecting 75 countries, have created significant anxiety within the healthcare sector.
The Impact of Visa Pauses and TPS Terminations
Five of the top 13 source countries for immigrant direct care workers are currently impacted by the federal visa pause. Furthermore, the Supreme Court’s June 2026 ruling, which allowed for the termination of Haiti’s TPS designation, places the status of thousands of essential workers in jeopardy.
Industry advocates argue that these policies are "self-inflicted wounds." If a significant portion of the workforce is removed due to status changes, the already strained nursing home and home health sectors will face a catastrophic labor shortage. As one industry expert noted, "The policy intent to restrict immigration is colliding directly with the demographic reality of an aging American population that has no other source of care."
Future Implications: Can the System Hold?
The current model of long-term care in the U.S. relies on a workforce that is underpaid, demographically marginalized, and increasingly restricted by federal policy. The implications are three-fold:
1. The Quality of Care Gap
When turnover rates are high due to low wages and high stress, the continuity of care is broken. For an elderly patient, having a different aide every week is not merely an inconvenience; it is a health risk. The inability to retain staff means fewer eyes on patients, leading to higher rates of medical errors and neglect.
2. Economic Burden on the States
As Medicaid is the primary payer for long-term care, any increase in the cost of care—driven by the need to raise wages to attract workers in a tightening labor market—falls directly on state budgets. States are already struggling to balance these costs against other competing fiscal priorities.
3. A Looming Demographic Cliff
The "Silver Tsunami"—the massive cohort of Baby Boomers entering their 80s and 90s—is only just beginning to crest. If the current workforce is already at a breaking point with 2.3 million workers, the math for the next decade suggests that the system will require hundreds of thousands of additional workers just to maintain the status quo.
Conclusion: Bridging the Gap
The 2024 ACS data serves as a warning signal. The direct care workforce is the invisible scaffolding upon which the dignity and health of millions of Americans rest. Policy decisions regarding immigration, wages, and training are not just abstract political debates; they are the determinants of whether a future American senior will be able to age in their own home or face a desperate, underserviced, or nonexistent care environment.
To avert a total collapse, policymakers must look beyond short-term political posturing. Addressing the "direct care crisis" will require a multi-pronged approach: professionalizing the role through better wages and benefits, creating sustainable pathways for immigrant workers who provide the bulk of this essential labor, and investing in the infrastructure of home and community-based care. Without these changes, the system will not only fail the workers who provide the care but also the millions of families who rely on them every single day.