The contraceptive implant stands today as the most effective reversible birth control method available to individuals of reproductive age. As a cornerstone of long-acting reversible contraception (LARC)—a category that also includes intrauterine devices (IUDs)—the implant offers a "set-it-and-forget-it" solution that bridges the gap between daily oral contraceptives and permanent sterilization. Despite its clinical superiority, the journey of the implant in the U.S. has been marked by historical controversy, technical innovation, and ongoing systemic challenges regarding access, affordability, and public awareness.
Main Facts: The Clinical Standard for Efficacy
At the heart of the implant’s clinical appeal is its extraordinary reliability. With a failure rate of just 0.05%, it is statistically more effective than any other reversible contraceptive currently approved by the Food and Drug Administration (FDA).
Unlike birth control pills, patches, or rings, which rely on consistent user adherence, the implant is entirely clinician-dependent for insertion and removal. Once placed, it requires no maintenance, effectively eliminating the risk of human error or non-use. The device, a small, flexible, hormone-releasing rod, is inserted under the skin of the upper arm. It works by suppressing ovulation and thickening cervical mucus to prevent sperm from reaching an egg.
While the implant is highly effective, its medical utility extends beyond pregnancy prevention. Many clinicians prescribe it to patients experiencing dysmenorrhea (painful menstrual cramps) or those seeking to regulate or lighten heavy menstrual cycles. Furthermore, while historical concerns existed regarding the use of hormonal contraception during breastfeeding, the latest clinical guidelines—including the 2024 U.S. Selected Practice Recommendations for Contraceptive Use—confirm that progestin-only methods like the implant do not negatively impact breastfeeding outcomes.
A Chronology of Innovation and Evolution
The history of the subdermal implant is a narrative of rapid medical advancement tempered by the lessons of early failure.
The First Generation: Norplant
In 1990, the FDA approved Norplant, the first generation of subdermal implants. Manufactured by Leiras Oy, the system consisted of six silicone capsules containing levonorgestrel, which were inserted into the upper arm and provided protection for up to five years. While revolutionary, the device faced significant backlash. Users reported complications, leading to widespread litigation against the distributor, Wyeth-Ayerst. By 2002, the product was discontinued in the U.S. market, creating a period of skepticism surrounding implant technology.
The Modern Era: Implanon and Nexplanon
The landscape shifted in 2006 when the FDA approved Implanon, a single, thin, plastic rod. This iteration represented a substantial design leap, as it was easier and faster to insert and remove than the multi-capsule Norplant system. In 2010, the manufacturer replaced Implanon with Nexplanon. This version included critical safety upgrades: it was made radiopaque, meaning it is visible on X-rays to ensure precise placement, and it featured a refined, ergonomic insertion device. Today, Nexplanon remains the sole contraceptive implant available in the U.S.
Recent Regulatory Shifts
In 2026, the FDA implemented critical updates to the provision of the implant. Most notably, the approved duration of use was extended from three to five years, reflecting enhanced clinical confidence in the device’s longevity. Simultaneously, the FDA moved the implant into the Risk Evaluation and Mitigation Strategy (REMS) program. This regulatory step ensures that the device is distributed only to clinicians who have undergone rigorous, in-person training, specifically addressing the rare but serious risks associated with improper insertion.
Supporting Data: Demographics and Utilization Trends
Despite strong recommendations from the American College of Obstetricians and Gynecologists (ACOG) and the American Academy of Pediatrics (AAP), the implant is still underutilized compared to other methods like the IUD, the pill, or sterilization.
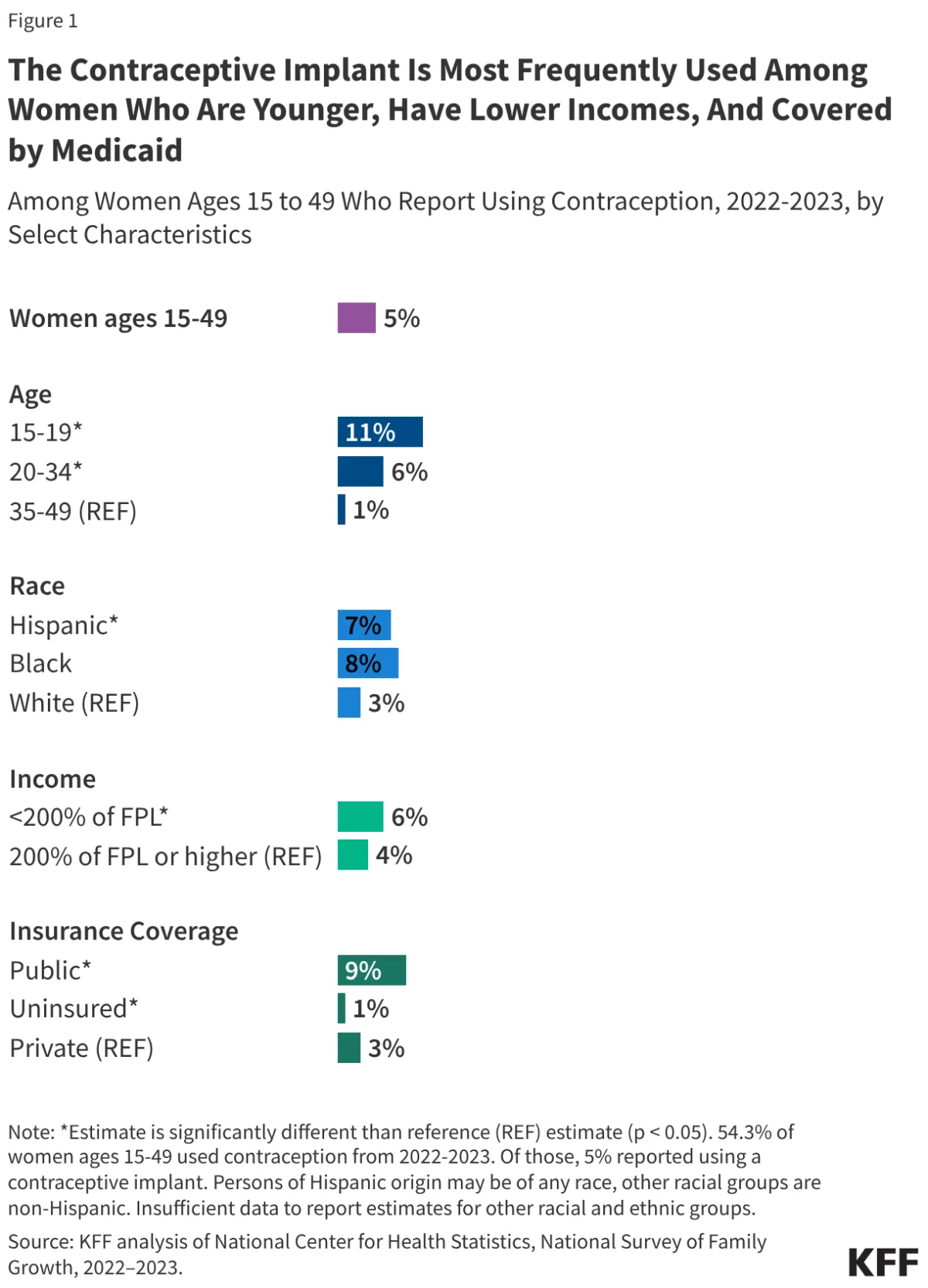
National data from 2022 to 2023 indicates that 5% of women aged 15–49 who use contraception utilize the implant. However, this usage is not evenly distributed across age groups. Approximately 11% of adolescent girls who use birth control choose the implant, compared to just 1% of women aged 35 to 49. This trend is likely driven by the desire for long-term pregnancy prevention, the convenience of a low-maintenance method, and the increased promotion of LARCs within youth-focused clinical settings.

Economic factors also play a significant role. Data shows higher implant utilization among lower-income populations and those covered by Medicaid. This correlation is largely attributed to the availability of these devices at publicly funded clinics, which often operate on a sliding scale or accept government-funded insurance, effectively removing the high upfront costs that can act as a barrier to care in private practice settings.
Official Responses and Clinical Barriers
The medical community has consistently advocated for increased access to LARCs, yet systemic barriers remain. A 2023 KFF survey revealed that while 83% of OBGYNs offer implants in their practices, barriers to entry persist.
The "Same-Day" Challenge
A significant hurdle is the requirement for multiple visits: one for counseling, another for insertion. ACOG strongly advocates for "same-day insertion" to minimize patient attrition. Progress is being made; in 2015, only 37% of publicly funded clinics performed same-day insertions. By 2023, that number had reached 69%. However, clinicians still cite high upfront costs—the wholesale price of the device is roughly $1,275—and reimbursement delays as significant challenges that discourage clinics from stocking the implant.
Training and Certification
The transition to the REMS program has heightened the training burden. To provide Nexplanon, clinicians must now register with the REMS program, pass a knowledge assessment, and complete a 90-minute in-person training session. While these measures prioritize patient safety, they also necessitate a time and financial commitment that may be difficult for small, rural, or under-resourced clinics to meet.
Implications: The Looming Crisis of Access
The financial framework of the implant is currently protected by the Affordable Care Act (ACA), which mandates that most private insurance plans and Medicaid expansion programs cover all FDA-approved contraceptives without cost-sharing. This policy has been instrumental in increasing LARC initiation since 2012.
However, the future of this access is uncertain. Recent research shows that even with the ACA mandate, some patients are experiencing out-of-pocket costs for related services, such as office visits, ultrasounds, and pregnancy testing. In 2023, over one-third of women with private insurance paid a median cost of nearly $17 for implant-related services, a figure that, while modest for some, acts as a deterrent for others.
The most profound implication concerns the uninsured population. Title X-funded clinics and community health centers have long served as the safety net for reproductive care. As the U.S. faces potential shifts in federal policy and a projected rise in the uninsured rate, the risk to reproductive autonomy is acute. Data indicates that one in five uninsured women of reproductive age has had to abandon their chosen birth control method due to cost—a rate four times higher than those with insurance.
The Patent Horizon
Currently, there is no generic alternative to Nexplanon, and Organon USA holds patents that prevent competition until 2027–2030. Without a generic version to lower the wholesale price, the financial burden on the public health system will continue to be a primary driver of inequitable access.
Looking Ahead
The contraceptive implant represents a triumph of modern medicine, offering an unparalleled level of freedom from the anxieties of unintended pregnancy. Yet, as this analysis demonstrates, the efficacy of the device is only as good as the systems that provide it. For the implant to reach its full potential as a public health tool, the medical community and policymakers must address the trifecta of barriers: the high upfront cost for clinics, the need for continued clinician training, and the fragility of insurance coverage for the most vulnerable populations.
As we look toward the next decade, the focus must shift from simply inventing more effective technologies to ensuring that the most effective methods already in existence are accessible to everyone, regardless of their zip code, income, or insurance status. Protecting reproductive autonomy will require sustained investment in public health infrastructure and a commitment to removing the financial and systemic hurdles that currently stand between patients and their chosen path to family planning.