The landscape of modern medicine is currently undergoing a paradigm shift. For decades, the primary objective of clinical intervention was the management of symptoms—a reactive approach to disease. Today, thanks to the maturation of gene and genome-editing therapies, medicine has entered a proactive era where the goal is to correct the root cause of illness at the molecular level. Central to this revolution are two distinct, yet complementary, methodologies: in vivo and ex vivo gene therapy. While both aim to rectify genetic malfunctions, their procedural execution, clinical application, and logistical hurdles are fundamentally different.
Main Facts: Defining the Two Approaches
At its simplest, the distinction between these two modalities is a matter of geography: where the genetic modification takes place relative to the patient’s body.
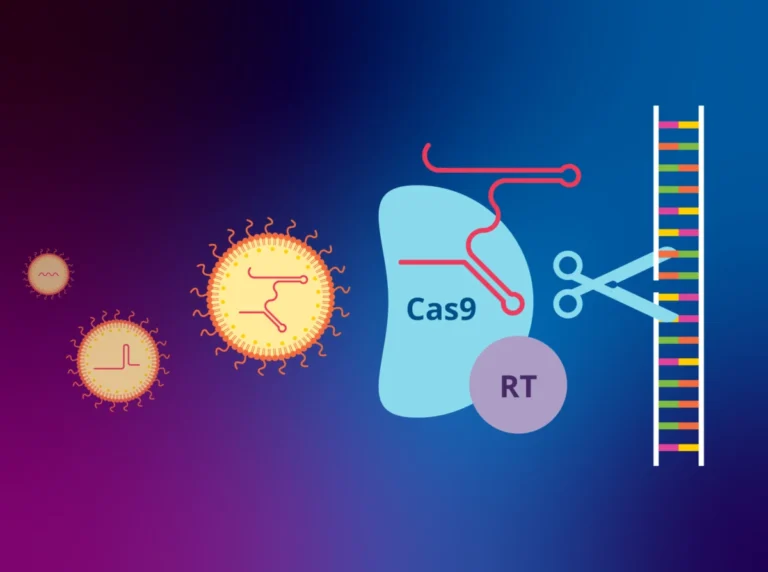
In vivo therapy involves the direct administration of a therapeutic agent—typically a viral vector or lipid nanoparticle carrying corrective genetic material—directly into the patient’s body. The target cells are modified while they remain in their natural biological environment. This approach is akin to a surgical strike on a specific organ or system, relying on the body’s internal circulatory or nervous systems to transport the treatment to the desired destination.
Conversely, ex vivo therapy is a multi-stage process that removes cells—often hematopoietic stem cells—from the patient. These cells are transported to a specialized laboratory, where they are genetically engineered under controlled, artificial conditions. Scientists introduce the therapeutic gene or use genome-editing tools, such as CRISPR, to rewrite a specific sequence. Once the modification is verified and quality control is assured, the "reprogrammed" cells are re-infused into the patient, where they theoretically integrate, proliferate, and begin to perform their corrected function.
A Chronology of Genetic Innovation
The trajectory of these therapies has been defined by rapid, often breathtaking, milestones in biotechnology.
The Early Days (1990s–2000s): The first attempts at human gene therapy were largely experimental and marked by both excitement and tragedy. Early clinical trials faced significant hurdles, particularly regarding the safety of viral vectors, which sometimes caused unintended immune responses.
The Turning Point (2010s): The development of more sophisticated viral vectors, such as adeno-associated viruses (AAVs), allowed for safer and more targeted delivery. During this period, the first therapies for rare, debilitating genetic disorders began to emerge from clinical pipelines.
The CRISPR Revolution (2020s–Present): The maturation of CRISPR-Cas9 technology shifted the field from merely "adding" functional genes to "editing" existing ones. The year 2023 served as a watershed moment when the UK’s MHRA authorized Casgevy, the world’s first CRISPR-based therapy for sickle cell disease and beta-thalassemia. This marked a shift from treating the symptoms of blood disorders to providing a potential functional cure.
Supporting Data: Clinical Utility and Targeted Conditions
The choice between in vivo and ex vivo is rarely a matter of preference; it is dictated by the anatomy and biology of the disease.
The Case for In Vivo
In vivo therapies are the gold standard for organs that are surgically inaccessible or biologically too sensitive to remove. For instance, the liver, the brain, and the retina represent "privileged" sites.
- Zolgensma (onasemnogene abeparvovec): Used to treat spinal muscular atrophy (SMA), this therapy delivers a functional copy of the SMN1 gene directly into the bloodstream to reach motor neurons.
- Luxturna (voretigene neparvovec): A landmark treatment for Leber congenital amaurosis, a degenerative eye condition. By injecting the vector directly into the subretinal space, clinicians can bypass systemic barriers to restore vision-critical protein production.
The Case for Ex Vivo
Ex vivo is the preferred route for conditions where cells can be easily extracted, modified, and expanded.
- CAR-T Cell Therapy: In the fight against certain blood cancers, clinicians extract T-cells from the patient, re-engineer them to recognize and attack tumor cells, and return them to the patient’s circulation.
- Hematological Cures: As demonstrated by Casgevy, blood disorders are ideal for ex vivo intervention because stem cells can be harvested from the bone marrow or peripheral blood, edited for precision, and successfully engrafted back into the patient.
Logistical and Economic Implications: The Scalability Gap
Perhaps the most significant differentiator between these two approaches is scalability.
In vivo therapies possess the inherent advantages of "off-the-shelf" drugs. Once a viral vector or lipid nanoparticle is manufactured, it can be stored, transported, and administered as a standard clinical infusion. While expensive to develop, the marginal cost of producing additional doses follows the traditional pharmaceutical model.
Ex vivo therapies, however, present a Herculean logistical challenge. Each patient represents an individual "batch." The process requires a high-tech manufacturing facility (often a "clean room"), specialized labor to handle the patient’s cells, and a sophisticated cold-chain logistics network to move biological material safely between the patient and the laboratory. This "bespoke" nature makes ex vivo therapies inherently more expensive and slower to scale, creating a bottleneck that healthcare systems like the NHS are currently grappling with.
Official Responses and Economic Reality
The cost of these "miracle" treatments has triggered a global debate on healthcare sustainability. With drugs like Libmeldy (for metachromatic leukodystrophy) carrying list prices exceeding £2.8 million, the question is not just how to innovate, but how to pay.
NHS England has taken a pragmatic, deal-making approach, often negotiating significant discounts with manufacturers in exchange for high-volume access to these therapies. These deals ensure that while the list price remains high, the actual expenditure is managed through confidential commercial agreements.
However, policy experts emphasize that the long-term solution lies in education. As genetic medicine becomes a standard of care, the burden of implementation falls on clinicians. The NHS Genomics Education programme has launched specialized courses for oncologists and general practitioners, aiming to demystify genomic testing and ensure that the right patients are identified for the right therapies at the right time.
Future Implications: The Path Toward "Universal" Genetic Care
The divide between in vivo and ex vivo will likely blur as technology advances. Researchers are currently working on in vivo genome editing—using nanoparticles to deliver CRISPR components directly to the bone marrow or other organs, potentially eliminating the need for the costly and complex ex vivo laboratory phase.
Furthermore, the rise of "universal" cell banks could simplify ex vivo therapies, moving them away from the patient-specific "autologous" model toward an "allogeneic" model (using healthy donor cells). This would drastically reduce costs and improve accessibility for patients in underserved regions.
As we stand on this precipice, it is clear that the transition from managing disease to curing it is no longer a matter of "if," but "how." The integration of these two modalities into the NHS and global health systems marks the beginning of a future where a genetic diagnosis is no longer a life sentence, but a targetable, treatable, and potentially reversible condition.
Disclaimer: This article is intended for informational and educational purposes only. It does not constitute professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider with any questions regarding a medical condition.