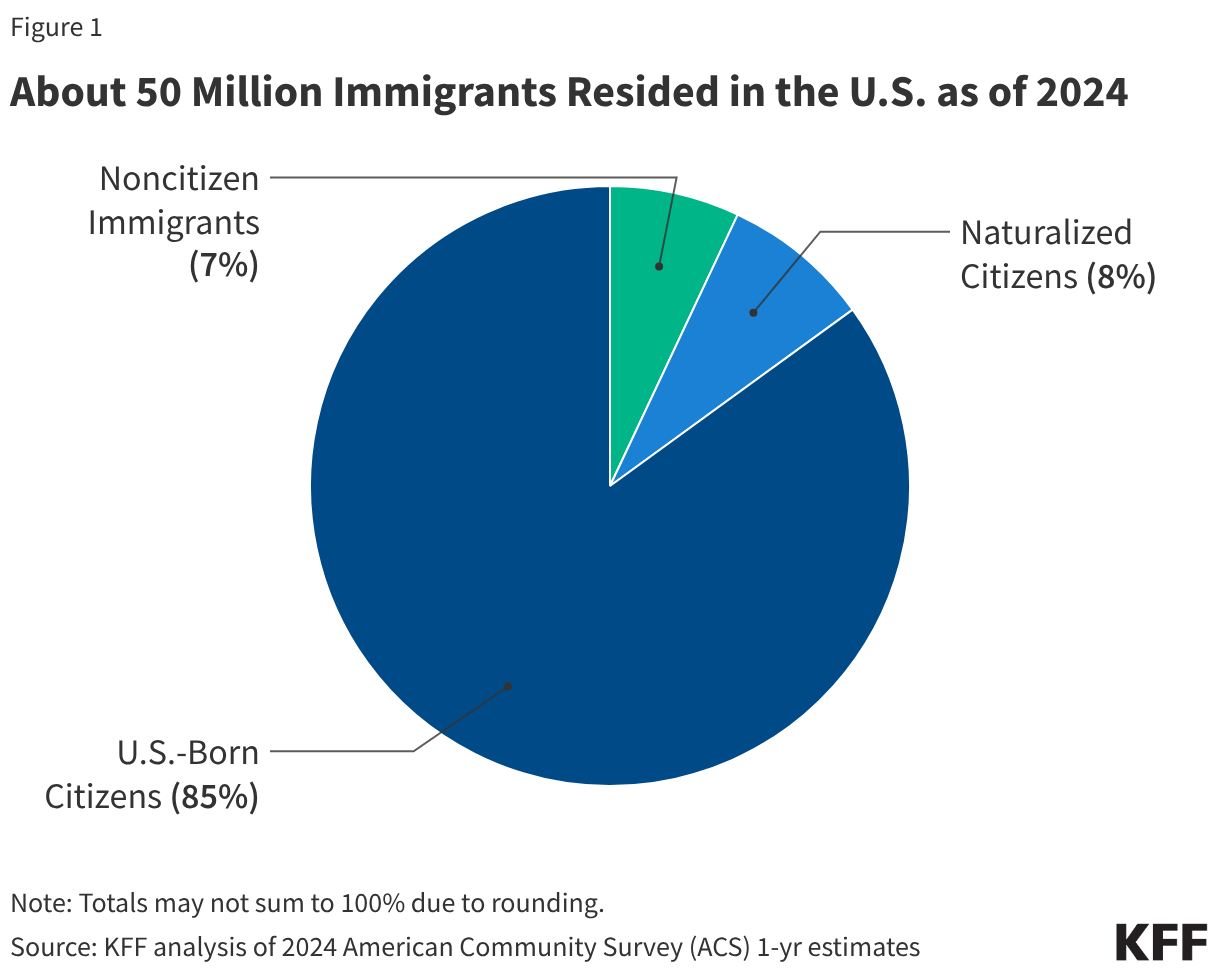
As of 2024, the United States is home to approximately 50 million immigrants, a diverse population that includes 24 million noncitizens and 26 million naturalized citizens. Together, these groups represent a significant portion of the nation’s demographic and economic fabric. However, recent federal legislative actions have fundamentally altered the landscape of healthcare access for this population, triggering a shift that experts warn could leave over a million individuals uninsured by the next decade.
This article provides an in-depth examination of the current state of immigrant healthcare, the impact of the 2025 reconciliation law, and the complex web of state-level responses currently unfolding across the country.

Main Facts: The Current Reality of Immigrant Health
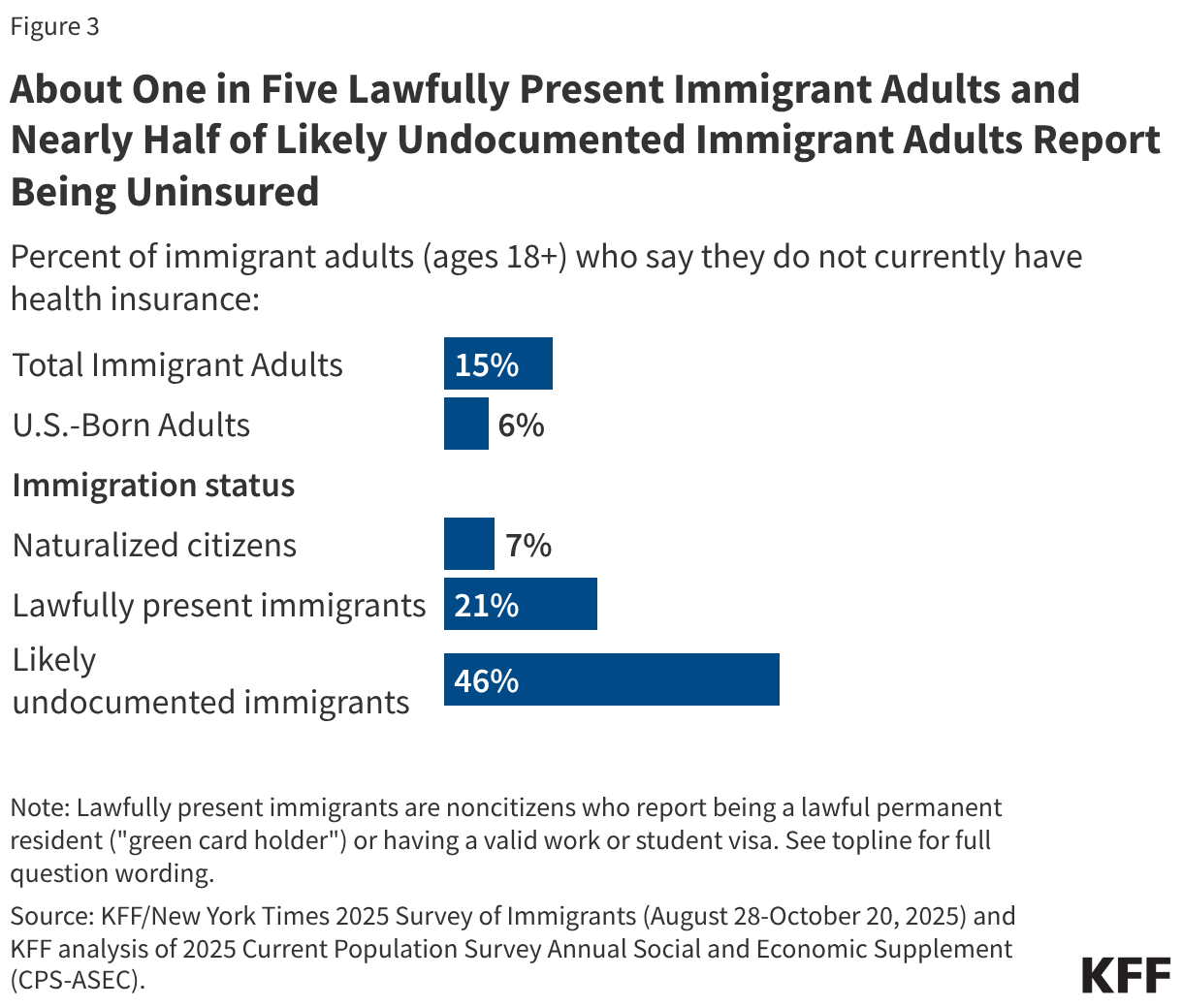
The immigrant experience in the U.S. is marked by significant disparities in health coverage. Data from the KFF/New York Times 2025 Survey of Immigrants reveals that while the majority of uninsured individuals in the U.S. are citizens, noncitizen immigrants face a much higher risk of being uninsured.
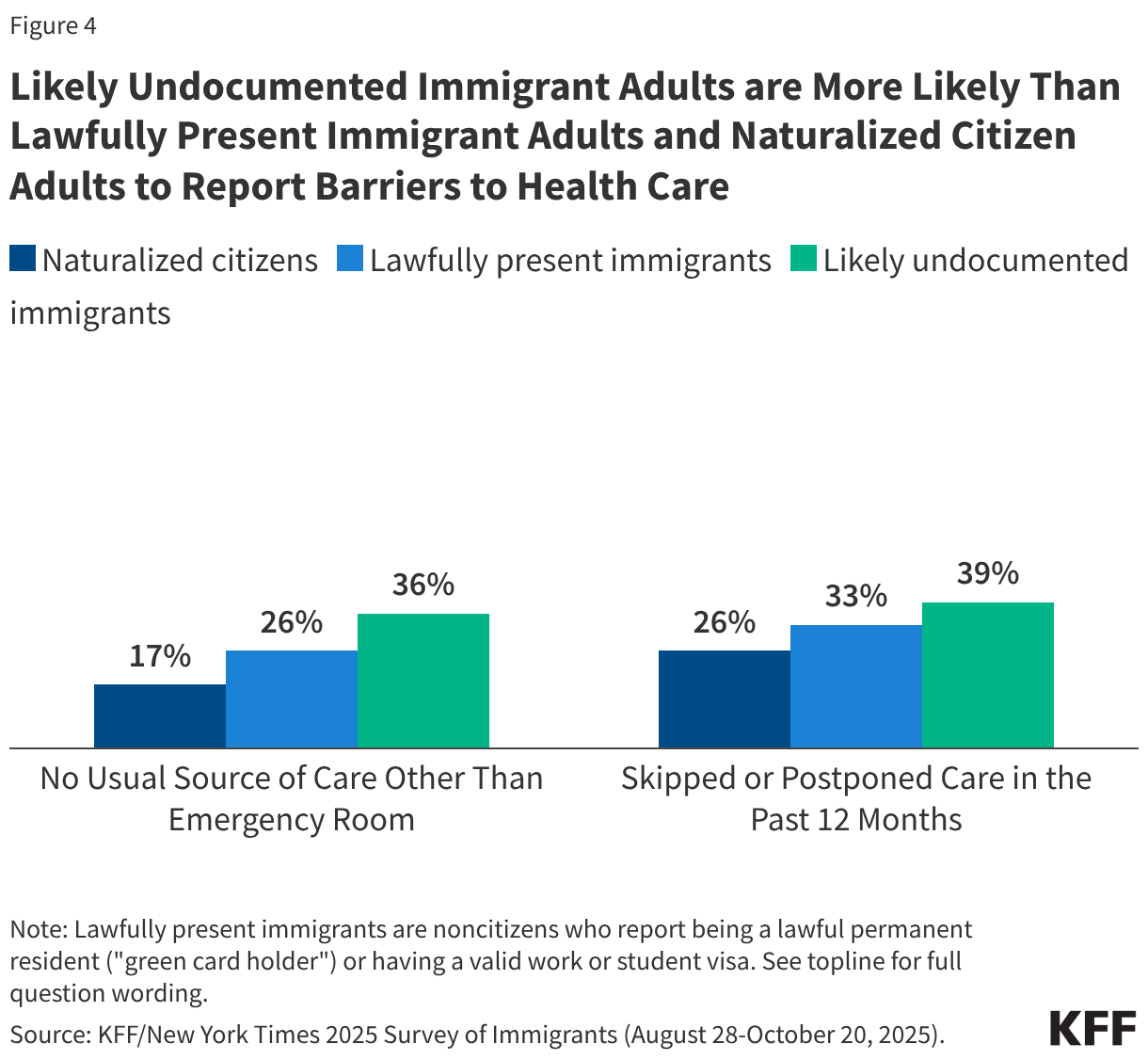
Nearly half (46%) of likely undocumented immigrant adults and one in five (21%) lawfully present immigrant adults report having no health coverage. In stark contrast, only 7% of naturalized citizens and 6% of U.S.-born citizens report being uninsured. These figures are not merely statistics; they translate into tangible barriers. Noncitizens, particularly those without authorization, are significantly more likely to postpone or skip necessary medical care, often resulting in complex, late-stage diagnoses that are more expensive to treat than preventative care.
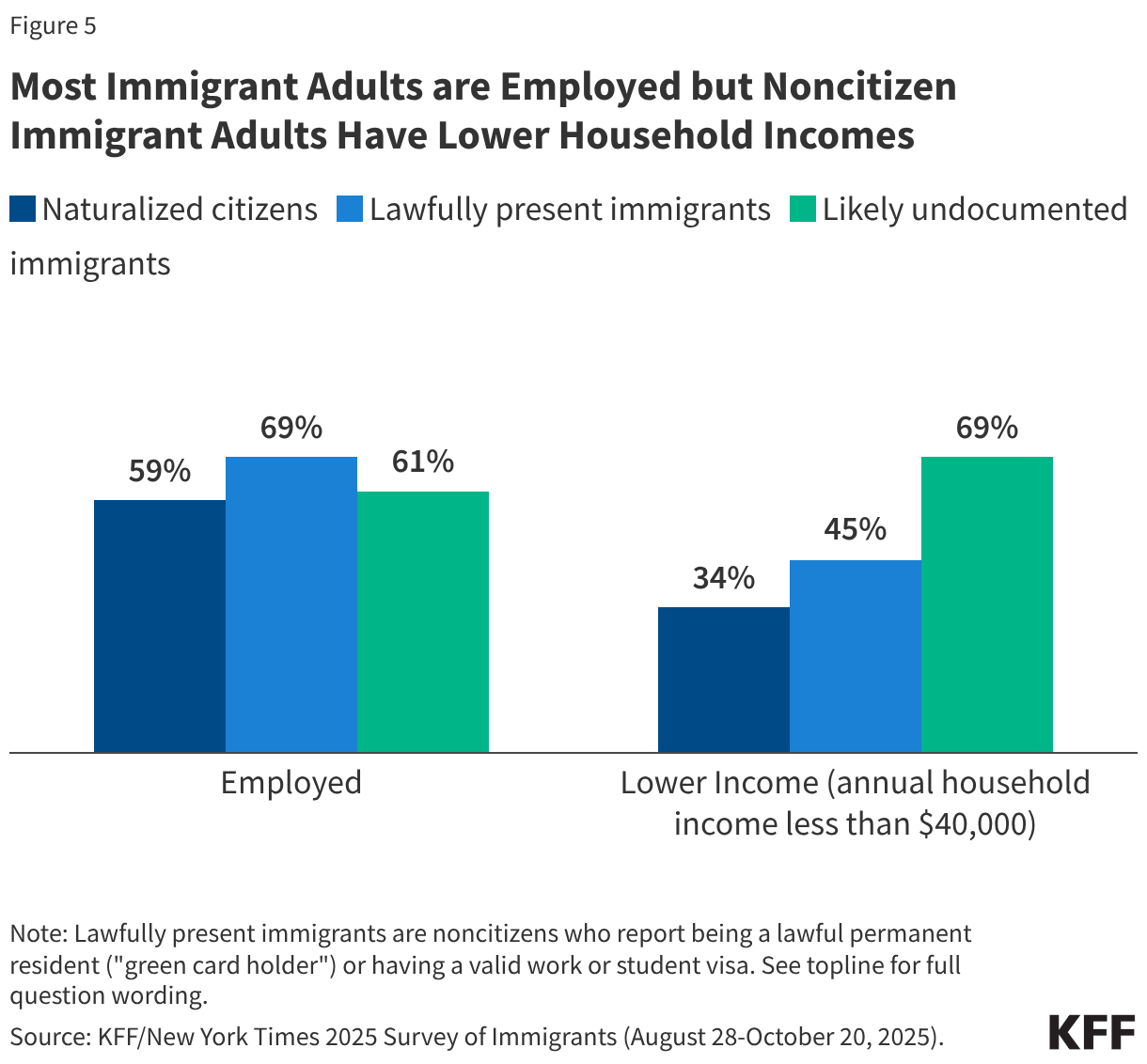
Paradoxically, while immigrants face the highest barriers to access, research consistently shows they utilize healthcare services at lower rates than their U.S.-born counterparts. Annual per capita health expenditures for immigrants are approximately 30% lower than those of U.S.-born citizens ($5,453 compared to $7,838). By contributing billions of dollars in taxes and insurance premiums while using fewer services, immigrants effectively subsidize the U.S. healthcare system, offsetting costs for the broader population.
Chronology of Legislative and Administrative Shifts
The path to the current healthcare climate for immigrants has been marked by a rapid succession of policy adjustments:
- Pre-2025: Lawfully present immigrants with "qualified" status (such as LPRs) could access Medicaid and CHIP, often after a five-year waiting period. Many states had begun to expand coverage for children and pregnant individuals regardless of immigration status.
- 2024: The Biden administration issued regulations to include DACA recipients in ACA Marketplace eligibility, aiming to reduce uninsured rates among "Dreamers."
- June 2025: The Trump administration published new regulations reversing the 2024 expansion, effectively rendering DACA recipients ineligible for ACA Marketplace coverage nationwide.
- January 1, 2026: Under the new 2025 reconciliation law, eligibility for tax credits for ACA Marketplace coverage was eliminated for lawfully present immigrants with incomes below 100% of the federal poverty level.
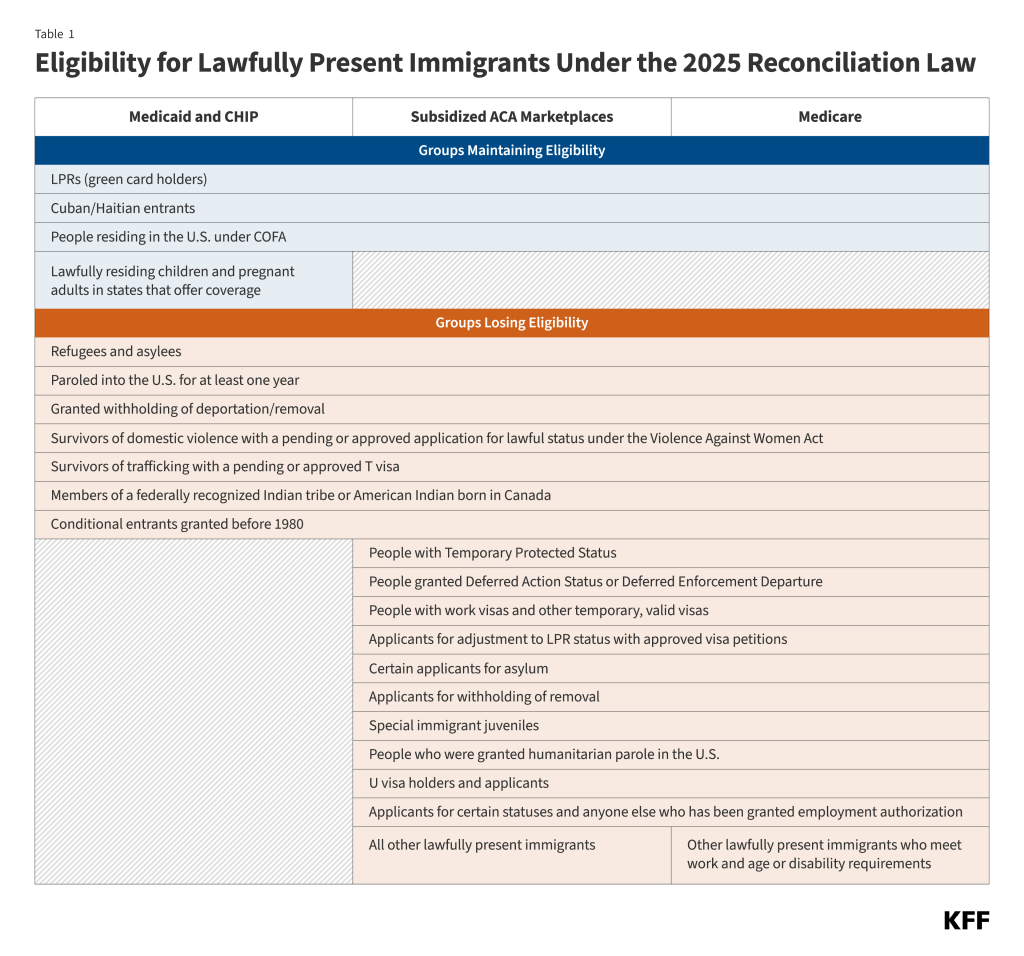
- October 1, 2026: Implementation of stricter Medicaid and CHIP eligibility rules, limiting access to a narrower group of immigrants (mostly LPRs, COFA migrants, and Cuban/Haitian entrants).
- January 4, 2027: The final deadline for current beneficiaries affected by the new restrictions to transition off federally funded coverage.
Supporting Data: The Impact of Eligibility Restrictions
The Congressional Budget Office (CBO) has projected that the 2025 reconciliation law will have profound consequences for health coverage. By 2034, an estimated 1.4 million lawfully present immigrants are expected to lose their health insurance.
The breakdown of this projected coverage loss is as follows:
- Medicaid/CHIP: 100,000 individuals.
- ACA Marketplace: 1.2 million individuals.
- Medicare: 100,000 individuals.
While the CBO estimates these measures will reduce federal spending by $131 billion and increase revenue by $4.8 billion over the next decade, public health advocates argue these savings come at a steep human cost. The restrictions specifically target groups previously considered "qualified," such as refugees and asylees who have not yet attained permanent resident status (green cards), forcing them into the ranks of the uninsured.
Official Responses and State-Level Maneuvering
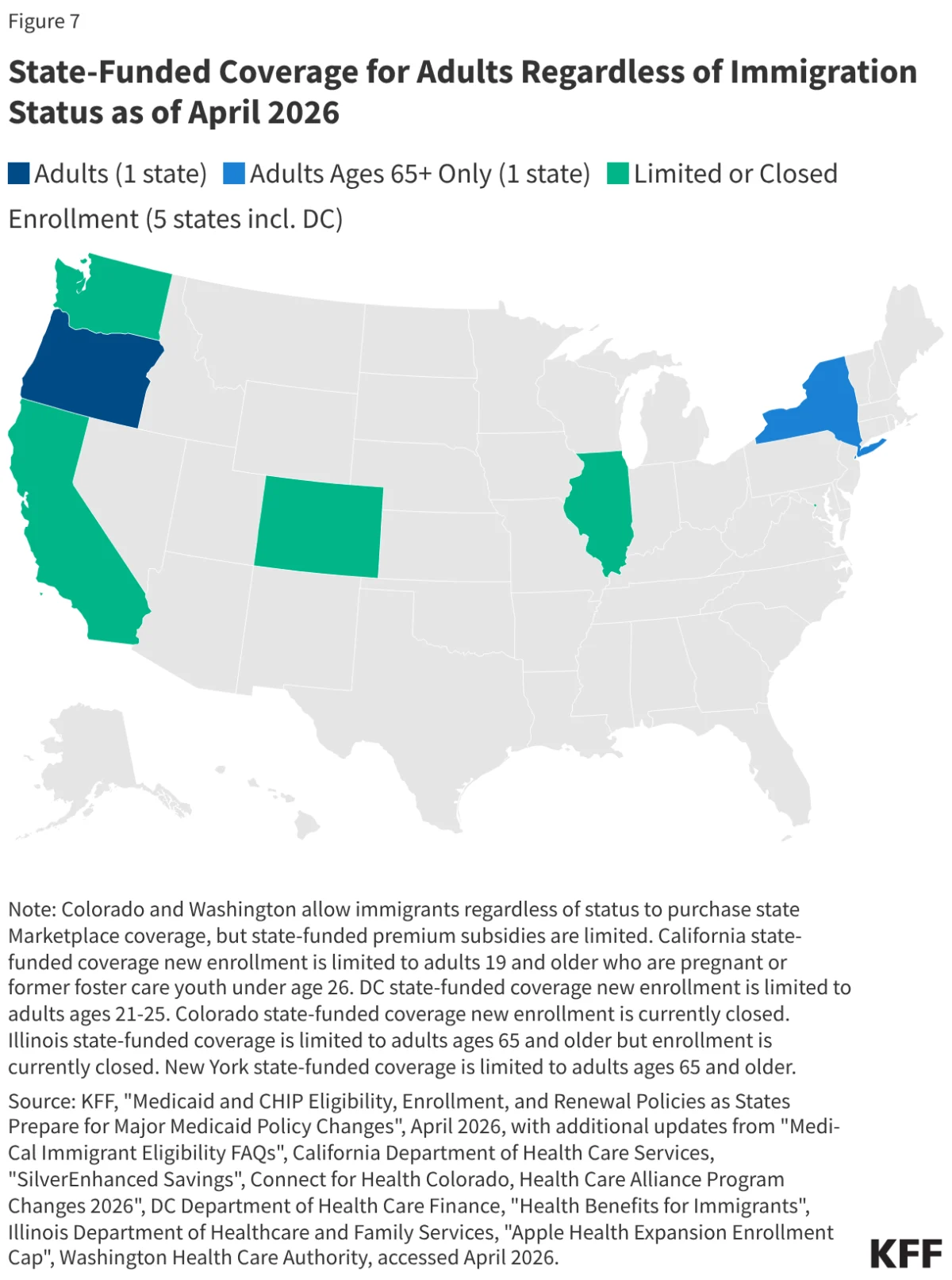
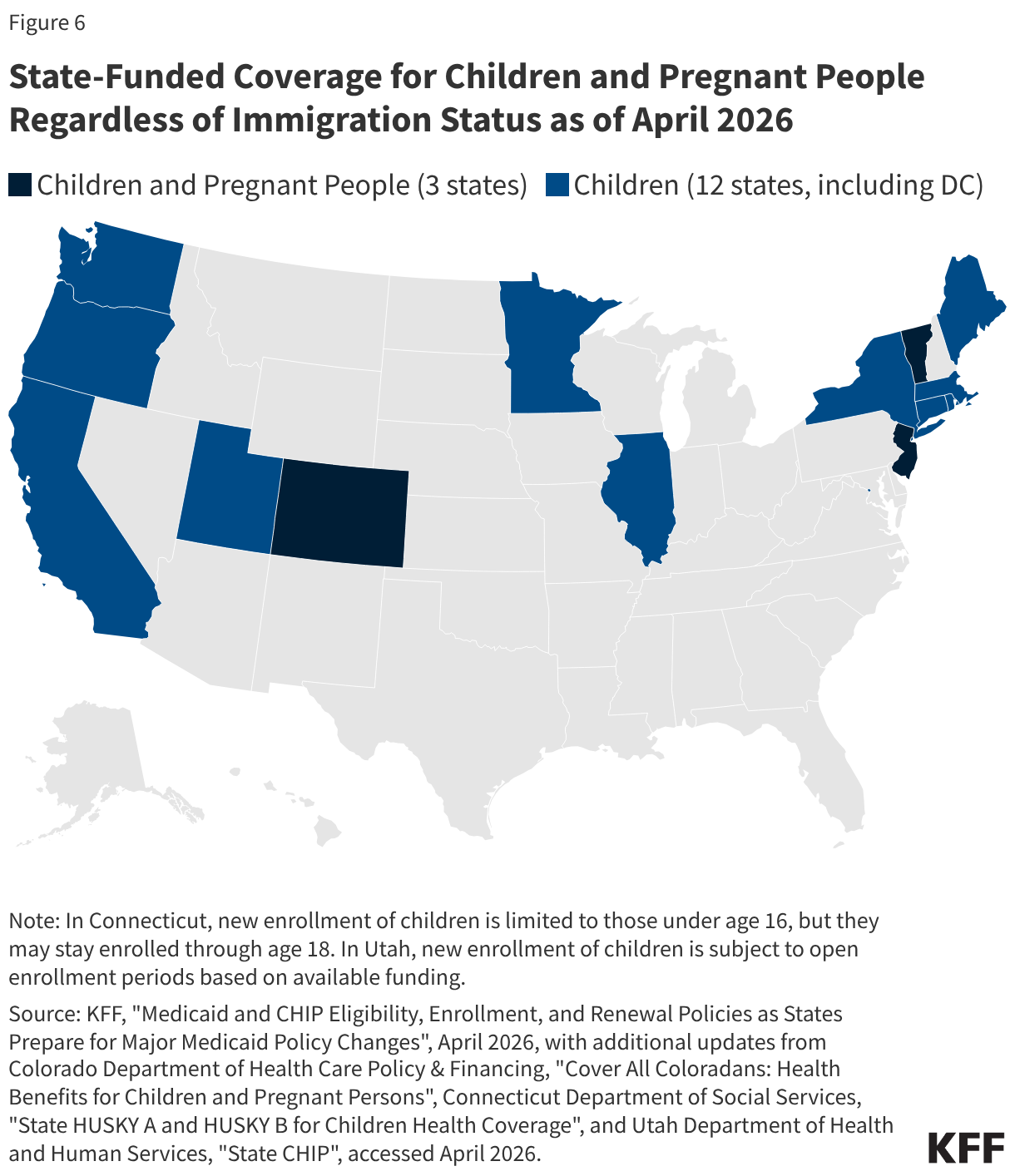
In the wake of federal retrenchment, the burden of ensuring healthcare access has shifted to the states. As of April 2026, 15 states and the District of Columbia provide state-funded comprehensive coverage to children regardless of immigration status. Seven states have also extended such coverage to income-eligible adults.
However, this is not a uniform trend. Fiscal pressures have forced a "patchwork" response:
- Rollbacks: States like Colorado are scaling back their state-funded programs, capping enrollment and limiting benefits due to budgetary constraints.
- Proactive Mitigation: New York and New Mexico have stepped in to fill the gaps created by the 2025 federal law, planning to use state funds to cover lawfully present immigrants who would otherwise lose their Medicaid or ACA Marketplace access.
- Legal Uncertainty: Many state legislatures are currently debating bills to further expand coverage, but their passage remains uncertain as states grapple with the administrative and financial requirements of replacing lost federal support.
Implications for Public Health and Safety
The implications of these policies extend beyond the individuals losing coverage. The KFF/New York Times survey highlights that fear is the primary driver of low enrollment, even among those who remain eligible.
The Climate of Fear
In 2025, 41% of immigrant adults reported worrying that they or a family member could be detained or deported, up from 26% in 2023. This environment of heightened immigration enforcement has caused a "chilling effect." Approximately 51% of immigrant adults, and nearly 78% of likely undocumented immigrants, expressed concern that healthcare providers might share their status with immigration enforcement officials. The introduction of new data-sharing agreements between the Centers for Medicare & Medicaid Services (CMS) and ICE has only served to solidify these fears, deterring families from seeking care for chronic conditions or preventative screenings.
Long-term Public Health Outcomes
The broader implications for the U.S. healthcare system are significant. When vulnerable populations avoid the doctor, they do not simply stop needing care; they delay it until it becomes a crisis. This shift toward emergency room utilization—which is more expensive and less effective at managing long-term health—places an increased strain on hospital systems.
Research has consistently shown that in states with more expansive coverage, immigrants are healthier, better integrated, and less reliant on emergency, uncompensated care. Conversely, as coverage is stripped away, public health experts anticipate rising rates of untreated chronic illness and increased postpartum health risks, as pregnant individuals lose access to consistent prenatal and maternity care.
The Economic Paradox
The legislative attempt to "save" federal dollars through these restrictions ignores the economic contributions of the immigrant population. By removing access to the ACA Marketplace—a system designed to pool risk—the government is effectively increasing the number of uninsured individuals who will inevitably rely on the "safety net" of public hospitals. This creates a cycle where the cost of care is shifted from insurance pools to local taxpayers and hospital systems, potentially undermining the very fiscal goals the 2025 reconciliation law aimed to achieve.
Conclusion
The U.S. is currently witnessing a historic retrenchment in how it views the role of the immigrant in its social safety net. With 1.4 million people set to lose coverage, the nation is at a crossroads. While some states are doubling down on inclusive healthcare policies as a matter of public health and economic efficiency, the federal trend toward restriction is creating a new, precarious reality for millions of residents. The coming years will reveal whether these state-level efforts can mitigate the damage or if the U.S. will see a permanent widening of health disparities that will impact the health and economic stability of communities across the country.