For over two decades, the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) has stood as the single largest commitment by any nation to address a specific disease. Since its inception in 2003, the program has been credited with saving an estimated 26 million lives, fundamentally altering the trajectory of the HIV/AIDS epidemic in sub-Saharan Africa and beyond. However, a groundbreaking new analysis by researchers at KFF and Boston University suggests that PEPFAR’s impact extends far beyond the fight against HIV. By acting as a cornerstone for broader health infrastructure, the program has served as a critical, albeit often unheralded, engine for improvements in maternal, child, and general health across the developing world.
Main Facts: The "Spillover" Effect
While PEPFAR is traditionally viewed as a "vertical" program—one laser-focused on a singular disease—this latest study indicates that its influence is distinctly "horizontal." By investing heavily in the building blocks of functional health systems, including workforce training, laboratory diagnostic capacity, and complex supply chain management, the program has bolstered the overall resilience of the health sectors in the countries where it operates.
The findings, which update previous research covering 2004–2018 to include data through 2022, reveal that PEPFAR-supported countries experienced significant, measurable improvements in all-cause mortality, maternal mortality, and child mortality compared to a control group of similar low- and middle-income nations. Perhaps most impressively, these gains occurred even as annual PEPFAR funding remained relatively flat for more than a decade, suggesting that the program’s integrated approach has yielded increasing "dividends" over time.
A Chronology of Impact: From 2004 to the COVID-19 Era
To understand the program’s evolution, one must look at its timeline.
- 2003–2004: PEPFAR is launched, marking the start of a massive influx of external health investment in the hardest-hit nations.
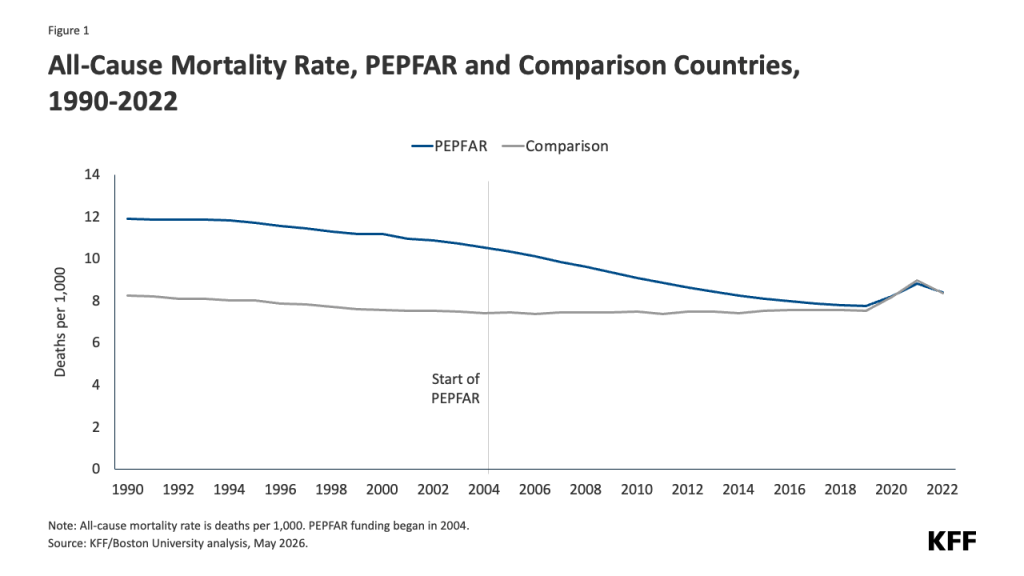
- 2004–2018: The initial study period. Researchers observed a stark divergence between PEPFAR-supported countries and the comparison group, characterized by a rapid decline in mortality rates in the former.
- 2019–2022: The COVID-19 pandemic era. This period presented a unique stress test for global health. The new data shows that while the pandemic caused temporary disruptions in health outcomes globally, these disruptions were widespread across all nations, not unique to PEPFAR recipients. Despite this global shock, the long-term trend of health improvement in PEPFAR countries remained robust.
Supporting Data: The Quantitative Case
The researchers employed a rigorous difference-in-difference, quasi-experimental design to compare 90 PEPFAR-supported countries against 67 control nations. The data reveals a compelling picture of health progress:
Mortality Reductions
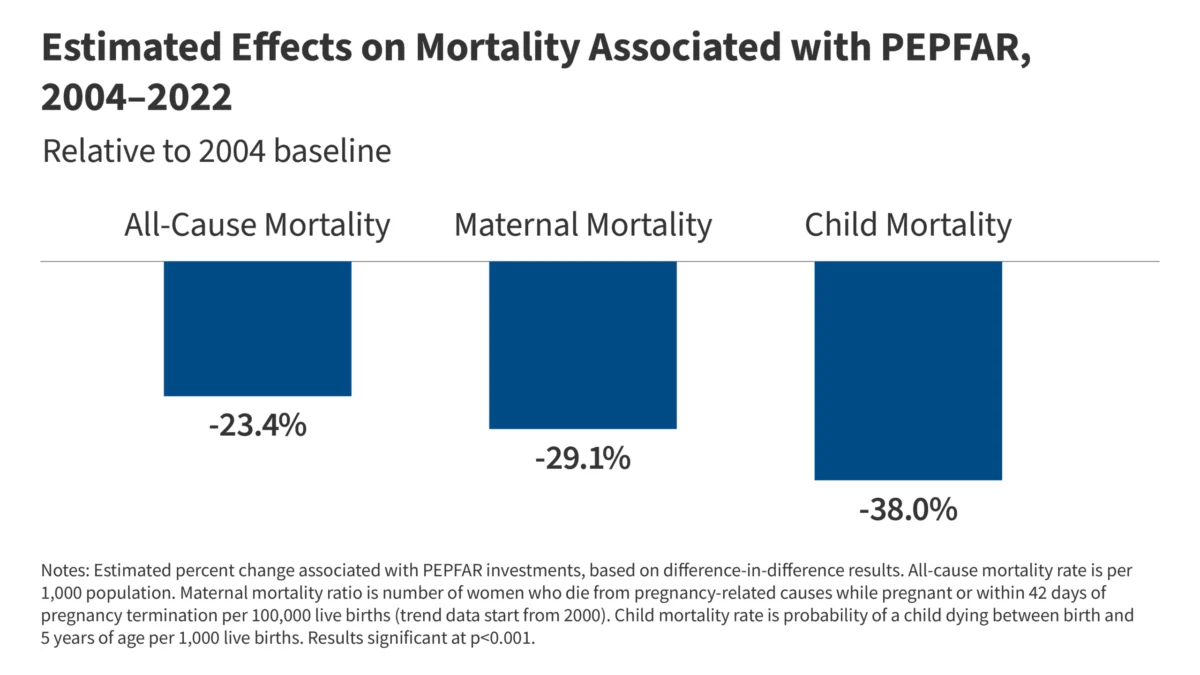
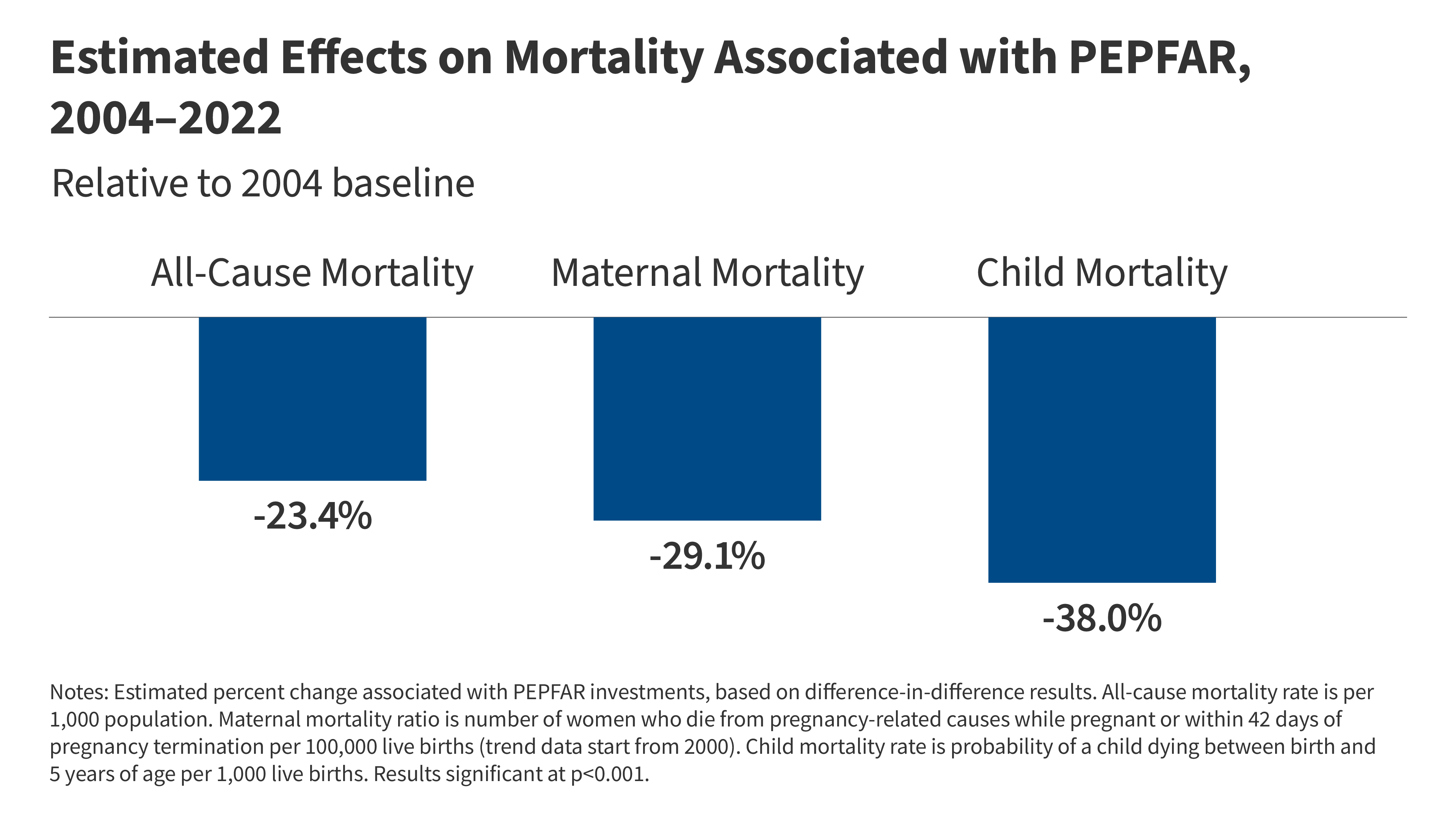
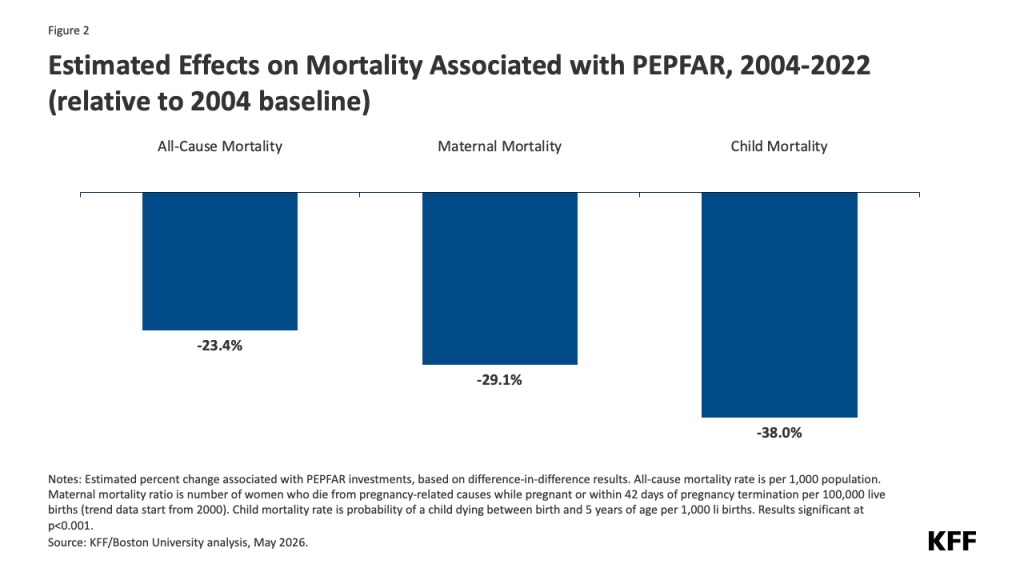
- All-Cause Mortality: PEPFAR investments were associated with a 23.4% reduction in the all-cause mortality rate between 2004 and 2022.
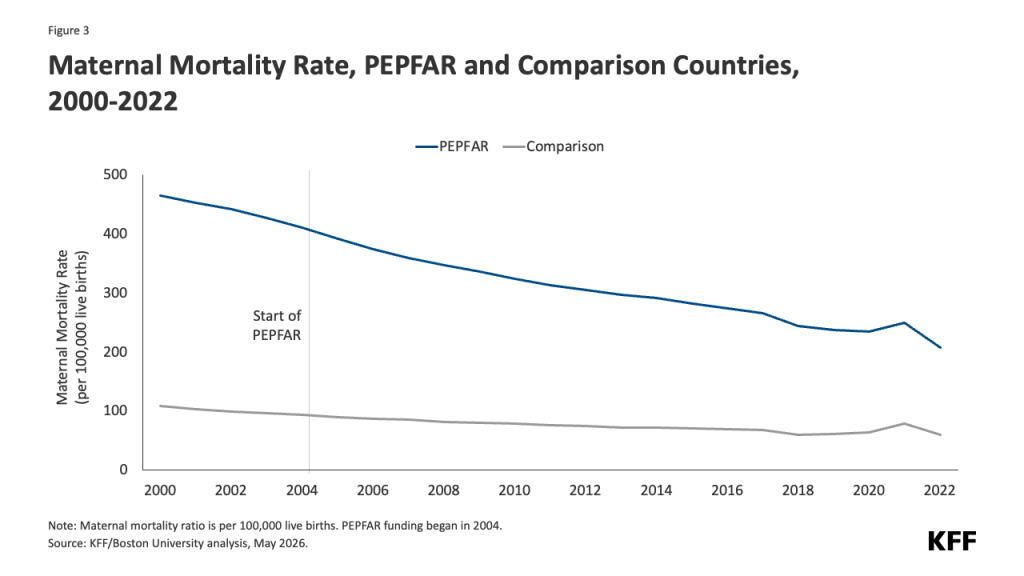
- Maternal Mortality: The maternal mortality ratio saw a significant decline of 29.1%.
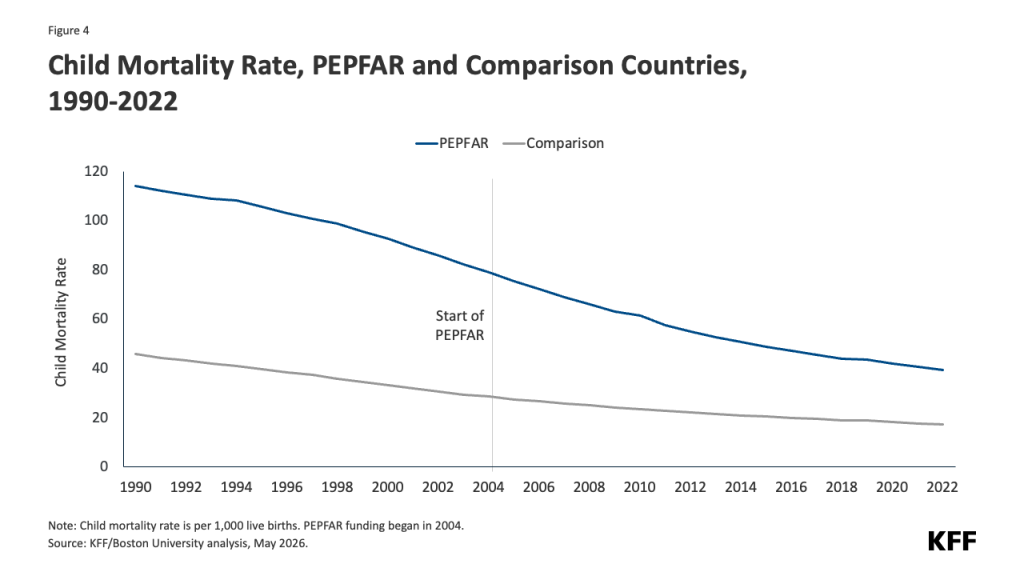
- Child Mortality: The most striking impact was seen in child health, with a 38.0% reduction in child mortality rates directly linked to the program’s presence.
Immunization Progress
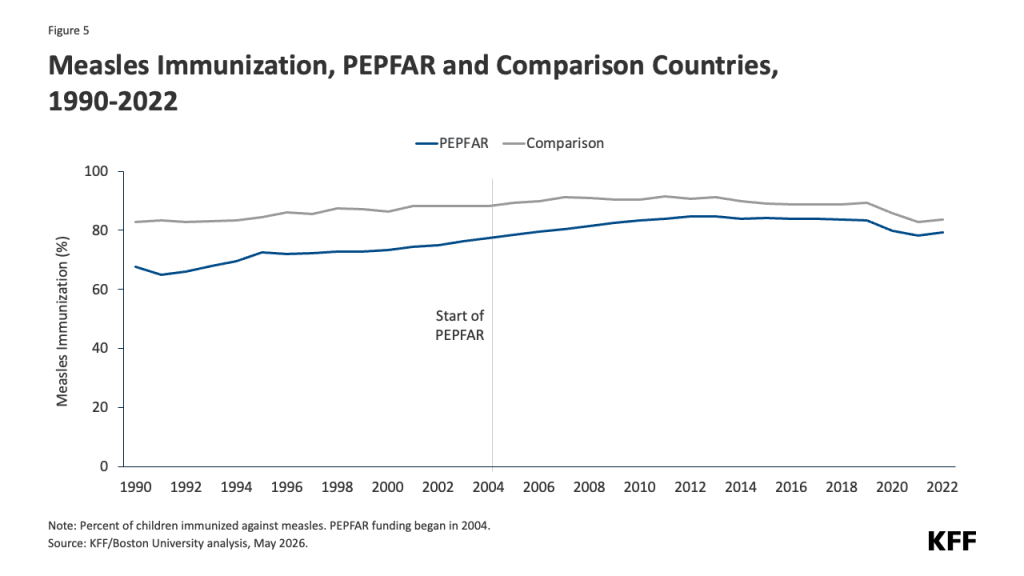
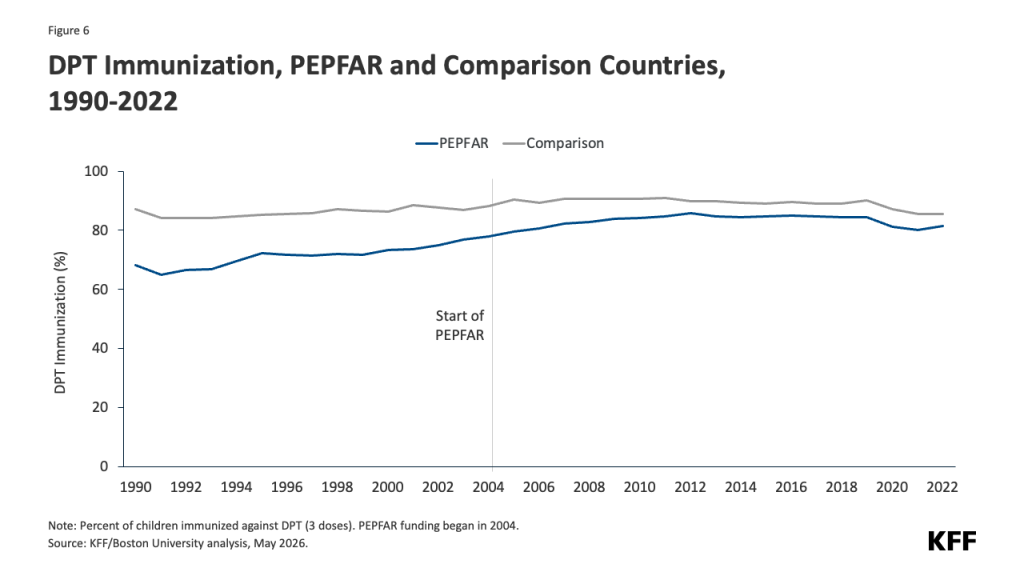
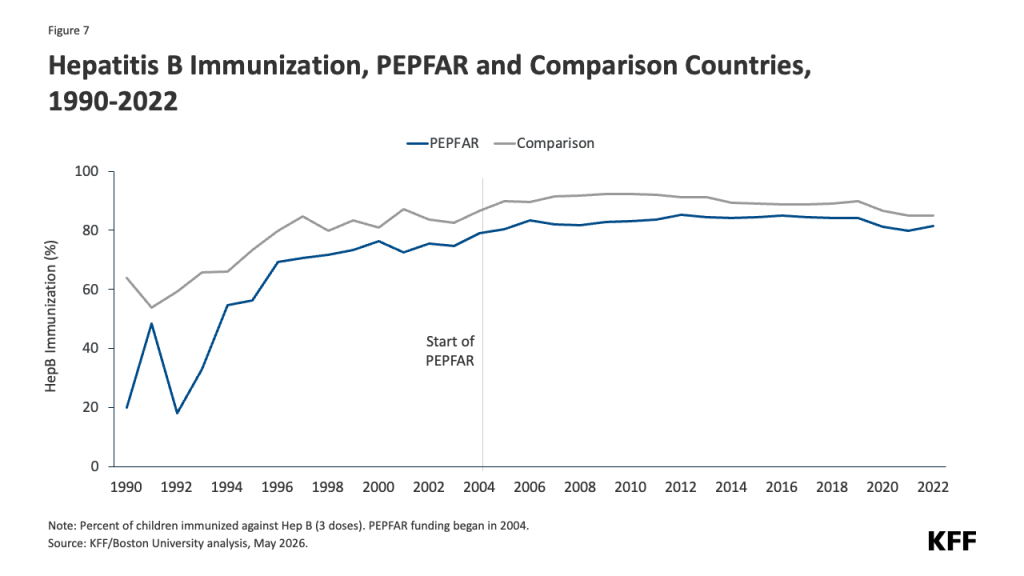
The integration of HIV services with primary care—such as reaching women during prenatal visits—has directly boosted immunization rates. The study highlights:
- Measles: A 9.0% increase in vaccination rates.
- DPT (Diphtheria, Pertussis, and Tetanus): An 11.4% increase.
- Hepatitis B: An 8.1% increase.
- Newborn Tetanus Protection: A 6.6% increase in protected births.
These figures are not merely statistical noise; they represent millions of children who avoided preventable diseases because the infrastructure built to combat HIV provided a vehicle for wider public health interventions.
The Role of Systemic Integration
Why has a program focused on a virus been so successful at addressing general health? The answer lies in the "platform effect." PEPFAR didn’t just buy medicine; it built the logistical "pipes" of healthcare.
In many of the countries analyzed, PEPFAR funding accounted for the majority of external health investment, frequently eclipsing domestic HIV spending. By establishing robust supply chains to deliver antiretroviral therapy (ART) to the most remote corners of the globe, the program effectively created a delivery system for other essential medicines. When a nurse is trained to manage an HIV patient’s regimen, that same nurse becomes more proficient at managing primary care for that patient’s family. When a laboratory is equipped to perform viral load testing, it is often repurposed to test for other pathogens, thereby improving the nation’s diagnostic capacity for future pandemics.
Official Responses and Political Context
The study arrives at a sensitive political moment. In recent years, debates regarding the future of U.S. global health funding have intensified. Specifically, policies pursued during the Trump administration involved significant scaling back of funding and services, with stated plans for further reductions.
Public health experts, including the authors of the KFF/Boston University study, warn that these shifts represent a high-stakes gamble. If the "platform" of PEPFAR is weakened—if laboratories are shuttered, supply chains are severed, or the healthcare workforce is reduced—the negative impacts will not be confined to HIV/AIDS. The data suggests that these cuts will likely have a "dampening effect" on the broader health gains observed over the last two decades.
While proponents of the funding reductions often cite the need for fiscal discipline or a shift toward domestic priorities, the empirical evidence suggests that the cost of these cuts will be measured in more than just HIV statistics. It will be measured in the reversal of the progress made in maternal survival, child health, and the general mortality rates of the world’s most vulnerable populations.
Implications for Future Global Health Policy
The study concludes with a sobering takeaway: the success of global health programs is often found in their secondary benefits. As international donors look toward the future, the PEPFAR model provides a blueprint for how to maximize limited resources.
However, the findings also highlight a vulnerability. The "incremental improvements" seen in successive phases of the program suggest that health progress is not a static achievement—it is a continuous process that requires sustained, long-term commitment. If the foundation—the health workforce and infrastructure—is neglected, the gains achieved in the last 20 years could easily erode.
Furthermore, the study addresses the potential for selection bias, noting that while their model controlled for variables like GDP, population size, and baseline disease prevalence, no statistical model is perfect. Yet, the consistency of the results across multiple specifications and the inclusion of robustness tests (such as running the model with and without demographic giants like China and India) lend significant credibility to the findings.
Ultimately, the analysis serves as a powerful reminder that in an interconnected global health landscape, programs do not exist in silos. By investing in the fight against HIV, the United States has inadvertently, but effectively, invested in the fundamental right to health for millions of people. As the debate over the future of PEPFAR continues in Washington and beyond, the data clearly signals that any move to dismantle this infrastructure carries a heavy price tag—one that will be paid by the most vulnerable in the form of higher mortality rates and weakened health systems.
The legacy of PEPFAR is currently at a crossroads. Will it continue to serve as the global standard for effective, integrated health investment, or will it be relegated to a historical success story whose decline mirrors the health outcomes of the nations it once supported? The evidence presented here suggests that the stakes are nothing less than the lives of millions.