

The landscape of American public health policy is undergoing a profound transformation. Under the provisions of the 2025 reconciliation law, a significant shift in Medicaid eligibility criteria is set to take effect nationwide. By January 1, 2027, states will be federally mandated to condition Medicaid coverage for adults in the Affordable Care Act (ACA) expansion group on meeting specific work requirements.
This policy pivot represents a departure from the previous decade’s regulatory environment and signals a new era of state-level autonomy—and obligation—in managing public health benefits. While the federal deadline provides a clear "hard stop" for implementation, the path to compliance is proving to be a complex, staggered process as states grapple with the choice between waiting for the federal deadline or pursuing early implementation strategies.
The Core Mandate: Understanding the 2025 Reconciliation Law
At the heart of the current policy shift is the 2025 reconciliation law, which codifies work requirements for the ACA Medicaid expansion population. Unlike previous iterations of work requirements, which were often contested through the administrative waiver process, these mandates are now baked into federal statute.
The law requires that non-exempt adults enrolled in the expansion group demonstrate active participation in the workforce, job training, or community service as a prerequisite for maintaining their health coverage. This transition is aimed at promoting self-sufficiency and aligning public health policy with labor market participation goals. However, the legislation grants states the flexibility to trigger these requirements before the 2027 deadline, provided they secure the necessary legal pathways through State Plan Amendments (SPAs) or Section 1115 demonstration waivers.
Chronology of Implementation: A Staggered Rollout
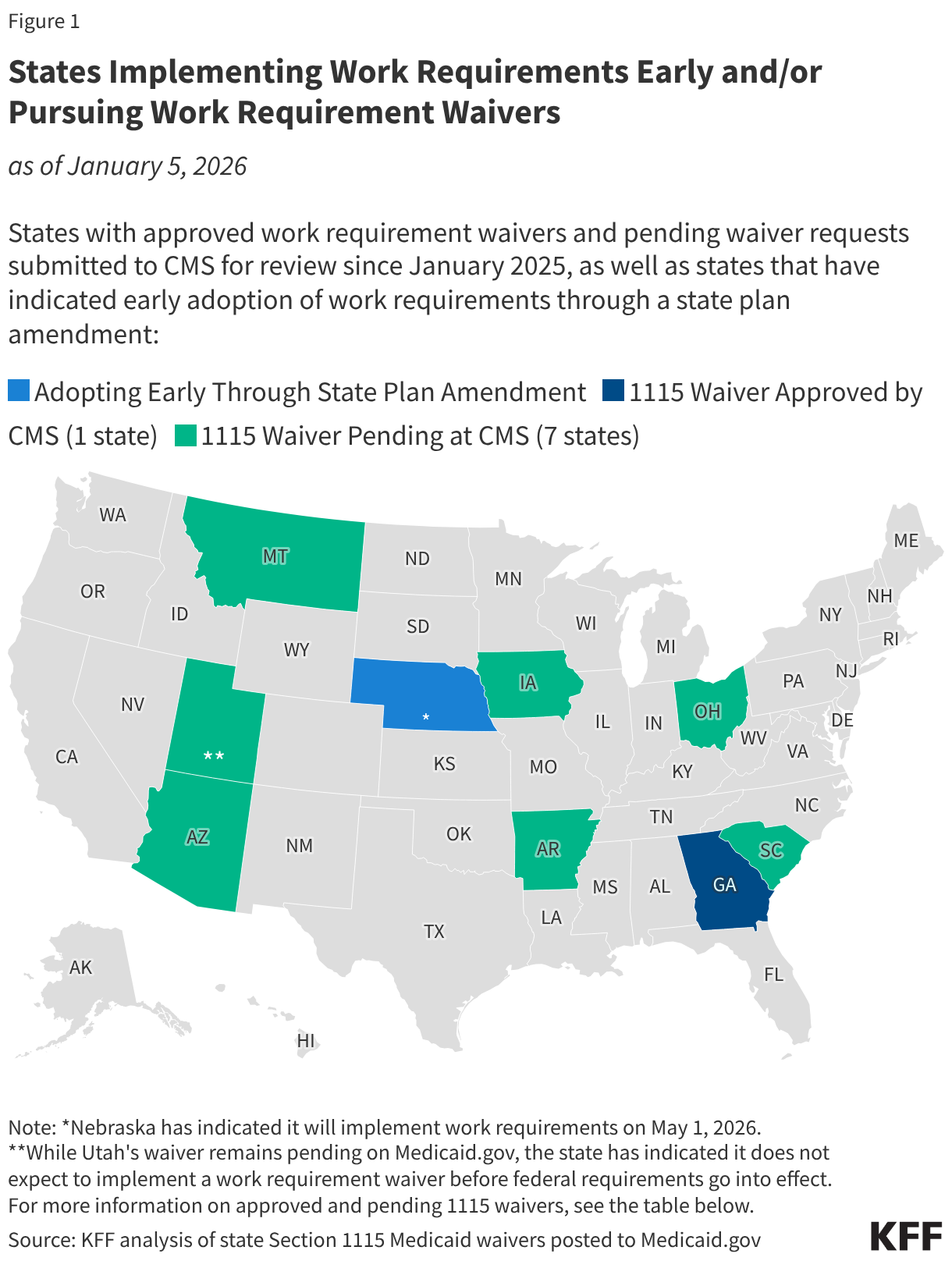
The timeline for implementation is no longer uniform across the United States. While the federal government has set the January 1, 2027, ceiling for universal compliance, several states have moved to accelerate this timeline.
Early Adopters: The SPA Strategy
State Plan Amendments (SPAs) have emerged as the primary vehicle for states looking to fast-track these requirements. By utilizing an SPA, states can modify their Medicaid programs to align with the new federal standards without the bureaucratic friction often associated with 1115 waivers.
- Nebraska: Leading the charge, Nebraska has announced a formal commencement date of May 1, 2026. This makes the state the first to officially transition its expansion population to the new federal work-requirement standards.
- Montana: Following closely, Montana has signaled its intent to enforce these requirements beginning July 1, 2026.
- Iowa: Rounding out the early adopters, Iowa has set its implementation target for December 1, 2026—just one month prior to the federal deadline.
The Waiver Landscape
Section 1115 waivers, which allow states to deviate from federal rules to test new models of care, have been the traditional battleground for work requirements. Since the inauguration of the second Trump administration, there has been a renewed surge in waiver applications. However, the landscape is shifting. Many states that initially sought 1115 waivers are now pivoting toward the more straightforward SPA route, or opting to wait for the federal law to take effect, thereby avoiding the uncertainty of CMS approval processes.
Supporting Data and Current Status
The current environment is characterized by a mix of legacy waivers and new, pending applications. The most notable outlier remains Georgia. Following protracted litigation regarding the Biden administration’s efforts to block the state’s work requirement model, Georgia remains the only state currently operating an active work-requirement waiver.
CMS recently granted a temporary extension for the "Georgia Pathways to Coverage" program. This extension, while allowing the program to continue, notably introduced new exemptions to the work requirements, reflecting a compromise between the state’s vision and federal oversight. Crucially, this extension is set to expire on December 31, 2026. On January 1, 2027, Georgia—like all other states—must fully align its programs with the uniform federal standards established by the 2025 reconciliation law.
Tracking the Shift
The transition is not just a matter of legislative intent; it is a complex logistical challenge for state health departments. States are currently re-evaluating their existing waiver applications to determine if they remain necessary. Some states are withdrawing pending 1115 applications as they realize the 2025 law renders their specific, bespoke work-requirement models redundant or legally precarious.
Official Responses and Administrative Guidance
The role of the Centers for Medicare & Medicaid Services (CMS) has become increasingly pivotal. While the federal law mandates compliance, the agency remains the arbiter of how states "bridge the gap" between now and 2027.
A central question facing policymakers is how CMS will treat 1115 waivers that seek to implement work requirements before 2027 while deviating from the specific parameters set in the new law. If a state’s 1115 proposal conflicts with the specific "flavor" of the federal law, CMS may reject the waiver, forcing the state to choose between adopting the federal model via an SPA or abandoning the early implementation goal.
State administrators have expressed a desire for clear, expedited guidance. In response, CMS has emphasized that while state flexibility is a cornerstone of the current administration’s approach, the "uniformity of the 2025 law" must remain the guiding star for all Medicaid programs.
Implications: The Road Ahead
The shift toward mandated work requirements carries significant implications for healthcare access, state budgets, and the social safety net.
Healthcare Access and Administrative Burden
Advocates for the policy argue that it incentivizes labor force participation, potentially improving the socioeconomic status of Medicaid enrollees. Conversely, critics and healthcare analysts warn of the "administrative cliff." Research into past work-requirement pilot programs suggests that the administrative burden of reporting hours can lead to "churn"—where eligible individuals lose coverage due to clerical errors or a failure to navigate complex reporting portals, rather than a failure to meet the actual work requirements.
Financial Impacts on States
For state governments, the fiscal implications are twofold. Implementing work requirements necessitates significant investment in tracking software, reporting infrastructure, and outreach to beneficiaries to ensure they understand the new rules. However, states may also see a reduction in Medicaid enrollment costs if a portion of the population is removed from the rolls due to non-compliance or if the requirement drives individuals into employer-sponsored insurance.
The Future of the Safety Net
The 2027 deadline will mark a historic change in the nature of Medicaid. Since its inception, the program has been primarily focused on providing a floor of coverage based on financial need. The move to add work requirements transforms the program into a hybrid model that balances health coverage with workforce development goals.
As we approach the 2027 threshold, the interaction between state-level innovation and federal oversight will define the success of these programs. The early implementation in states like Nebraska, Montana, and Iowa will serve as a bellwether for the rest of the country. These states are essentially acting as the testing ground for the national rollout, providing data on how to effectively communicate new requirements to beneficiaries and how to manage the transition without causing significant, unintended drops in coverage.
Conclusion: A New Paradigm
The 2025 reconciliation law has effectively ended the era of "wait and see" regarding Medicaid work requirements. By enshrining these mandates in federal law, the legislative branch has shifted the debate from whether work requirements should exist to how they will be implemented most effectively. As states prepare for the January 2027 deadline, the focus will inevitably turn toward the efficacy of these programs in achieving their dual goals: promoting employment and maintaining the integrity of the public health safety net. The coming months will be critical, as states finalize their SPAs and navigate the final stages of the 1115 waiver process, setting the stage for a nationwide transformation of the Medicaid program.







