In the landscape of American healthcare, a silent but significant transformation is underway. For decades, the U.S. has operated with a bifurcated approach to health: Medicaid serves as the primary insurance vehicle for 80 million low-income individuals, while a decentralized public health infrastructure works to monitor, prevent, and mitigate threats at the community level. While these two systems share the same patient populations and overlapping goals, they have historically functioned as siloed entities.
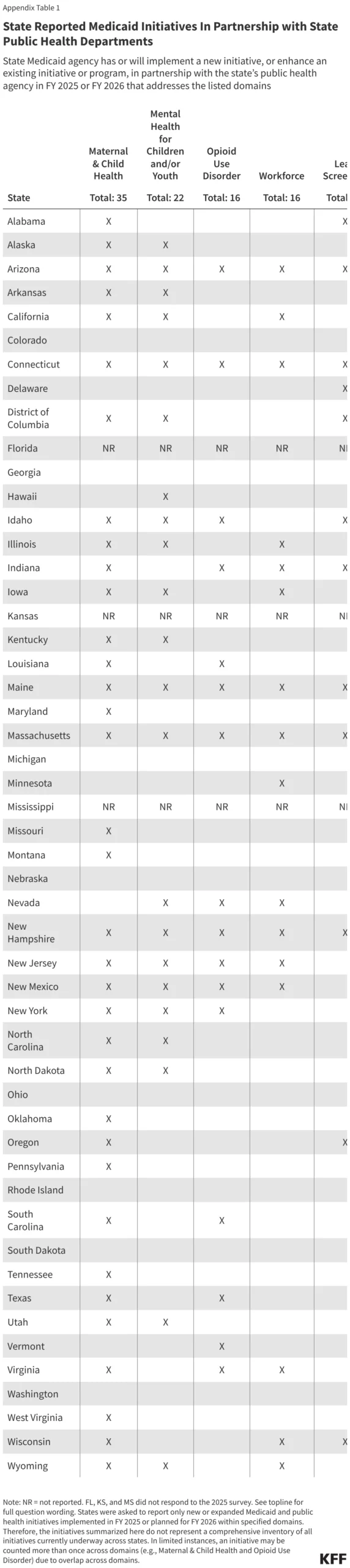
However, findings from the 25th annual Medicaid budget survey—conducted by KFF and Health Management Associates (HMA) in collaboration with the National Association of Medicaid Directors (NAMD)—reveal a growing momentum toward integration. Over three-quarters of responding states have launched or expanded formal partnerships between Medicaid and public health agencies in Fiscal Year 2025 and planned for 2026, marking a pivotal shift in how the nation approaches the social and clinical determinants of health.
The Structural Divide: Why Alignment Matters
To understand the significance of these initiatives, one must recognize the inherent difference in the two systems’ mandates. Medicaid is a clinical insurance program; its statutory power is limited to funding specific, medically necessary services for eligible, enrolled individuals. Conversely, the U.S. public health system is a community-wide guardian. It is tasked with surveillance, population-level disease prevention, and the enforcement of policies that protect the environment and social fabric.
"Public health serves entire communities, not just insured individuals," the KFF/HMA report notes. "Medicaid agencies and public health departments often work toward similar priorities, but there has historically been a lack of strong, sustained partnership."
The consequences of this fragmentation are profound. When Medicaid and public health agencies do not communicate, the safety net develops holes. Data sharing is delayed, outreach efforts are duplicated, and the resources meant to protect the most vulnerable are spread thin. By bridging this gap, states aim to create a cohesive ecosystem that manages care from the individual to the population level.
Chronology of the Shift: From Isolation to Integration
The impetus for this collaboration has been accelerated by the lessons of recent public health crises, including the COVID-19 pandemic and the ongoing opioid epidemic.
- Pre-2024: Cooperation was largely ad-hoc, often triggered by emergency response needs rather than systemic policy design.
- FY 2025: A marked shift occurred as state budget cycles began prioritizing "integrated health" as a cost-saving and outcomes-driven strategy. States began formally embedding public health outreach within Medicaid service delivery.
- FY 2026 Outlook: States are currently in the planning stages for even deeper integration, particularly in the realms of mental health, rural healthcare access, and advanced data interoperability.
This survey represents a snapshot of this evolution, focusing on initiatives either implemented or expanded during this window. While the report acknowledges that it does not capture the entirety of legacy partnerships, the volume of new initiatives confirms that "collaboration" is no longer just a buzzword—it is a budgetary priority.
Supporting Data: Key Domains of Collaboration
The survey highlights five primary domains where Medicaid and public health are finding common ground: Maternal and Child Health, Children’s Mental Health, Opioid Use Disorder (OUD), Lead Screening, and Infectious Disease.
Maternal and Child Health
With Medicaid covering 41% of all births in the U.S., the maternal health crisis is a primary driver for integration. Public health agencies, which hold the keys to surveillance and community-based doula programs, are now partnering with Medicaid to ensure that prenatal and postpartum care extends beyond the clinical office. By leveraging public health’s community outreach, Medicaid can better track high-risk pregnancies and ensure that interventions—such as nutrition support and mental health screenings—are accessible to those in "health deserts."
Children’s Mental Health
As adolescent mental health emerges as a national emergency, the role of the school as a point of care has become vital. Nearly one in five public school students utilizes school-based mental health services. States are increasingly utilizing Medicaid to fund these services, while public health departments provide the framework for early detection and teacher/caregiver training. This synergy transforms the schoolhouse into a legitimate extension of the healthcare system.
The Opioid Crisis
The opioid epidemic claimed over 79,000 lives in 2023. Medicaid covers nearly half of all adults with Opioid Use Disorder (OUD). The new wave of partnerships focuses on "harm reduction"—distributing naloxone and fentanyl test strips through public health channels while ensuring Medicaid provides the financial backbone for long-term medication-assisted treatment (MAT).
Lead Screening and Environmental Health
Federal law mandates lead screenings for children in Medicaid, yet adherence remains uneven. Public health departments are now using their environmental data to flag "hot zones" for lead exposure, allowing Medicaid programs to prioritize targeted outreach and diagnostic testing for children in the most at-risk neighborhoods.
Infectious Disease
Vaccine-preventable disease outbreaks have underscored the fragility of public health. By aligning the CDC-funded "Vaccines for Children" program with Medicaid’s provider networks, states are creating a dual-track system: public health handles the surveillance and outreach, while Medicaid handles the billing and provider reimbursement, ensuring that no patient slips through the cracks of the clinical-public health divide.
Official Perspectives: The NAMD and Policy Outlook
According to Cory Caldwell, Senior Policy Analyst at the National Association of Medicaid Directors (NAMD), the move toward integration is not merely about convenience; it is about fiscal survival and clinical efficacy. "Medicaid agencies and public health departments are beginning to realize that they are two sides of the same coin," Caldwell notes.
State Medicaid directors surveyed by KFF/HMA emphasized that the biggest hurdle remains "system fragmentation." Many directors reported that while the political will exists, the technical barriers—such as disparate data systems that cannot "speak" to one another—remain a significant challenge. The push for 2026 is largely centered on overcoming these technical hurdles through centralized data-sharing platforms.
Implications: A New Era for the Healthcare Safety Net
The movement to bridge Medicaid and public health has far-reaching implications for the American healthcare system.
- Efficiency and Cost-Reduction: By coordinating efforts, states can avoid the duplication of services. When public health and Medicaid share data, they can identify high-need individuals before they end up in the emergency room, saving significant long-term costs.
- Addressing Social Determinants of Health (SDOH): Public health agencies are better equipped to address non-clinical factors like housing, nutrition, and environmental hazards. By integrating these departments, Medicaid can begin to address the root causes of illness rather than just the symptoms.
- Rural Health Resilience: Rural communities, which often lack specialized care, stand to benefit most. Mobile clinics and community health worker (CHW) programs, jointly funded by public health grants and Medicaid reimbursement, offer a sustainable model for keeping rural healthcare viable.
- Health Equity: Disparities in health outcomes are often a byproduct of the gaps between these two systems. A unified approach allows for more equitable distribution of resources, as data-driven decisions replace guesswork in the allocation of state health funding.
Conclusion: The Road Ahead
The integration of Medicaid and public health is a slow, structural shift, but it is an essential one. As states look toward the end of 2026, the focus will likely shift from initial implementation to scaling these successes. The challenge will be to maintain this momentum in an era of fiscal tightening.
If states can successfully weave together the clinical power of Medicaid with the community-based mandate of public health, the result will be a more resilient, proactive, and equitable healthcare system. The findings from the 25th annual budget survey suggest that for the first time in recent history, the walls between these two vital institutions are beginning to crumble, replaced by a collaborative framework designed to serve the American public as a whole, rather than as a collection of fragmented parts.