A recent study published in the medical journal Cancers (2026) has introduced a critical shift in how clinicians manage non-medullary thyroid carcinoma (NMTC). Researchers from the University of Siena, Italy, have determined that patients with a familial history of the disease—known as familial NMTC (fNMTC)—experience a significantly less stable "excellent response" to treatment compared to their sporadic counterparts.
The study, which analyzed 795 patients over several decades, suggests that while familial cases are not inherently more aggressive in terms of structural progression, they are prone to biochemical fluctuations that necessitate a move away from standard monitoring toward more prolonged, vigilant surveillance.
Main Facts: The "Fragility" of Remission
Dynamic risk stratification (DRS) has become the gold standard for managing differentiated thyroid carcinoma. By integrating biochemical, structural, and imaging data over time, doctors can adjust their surveillance intensity based on how a patient responds to their initial surgery and radioiodine treatment.
The research, led by Dr. Laura Valerio and Dr. Maria Grazia Castagna, discovered that familial status is an independent predictor of "losing" an excellent response. While an excellent response is typically viewed as a permanent hallmark of remission, patients with fNMTC were found to be more than three times more likely to lose this status compared to those with sporadic disease (sNMTC).
Crucially, the "worsening" of the disease in familial cases was rarely structural. Instead, it was defined by indeterminate biochemical markers or rising levels of thyroglobulin (Tg) without clear evidence of cancer recurrence on imaging. This indicates that while the disease is not necessarily "deadlier" in a structural sense, it is significantly more "volatile."

Chronology: A Longitudinal Look at Thyroid Health
The research team conducted a retrospective study spanning over three decades (1990–2021), focusing on 795 patients. The methodology was structured around two key temporal snapshots:
- Initial Assessment: Evaluated 6–12 months post-initial therapy.
- Last Outcome: Evaluated after a median follow-up of 12.6 years.
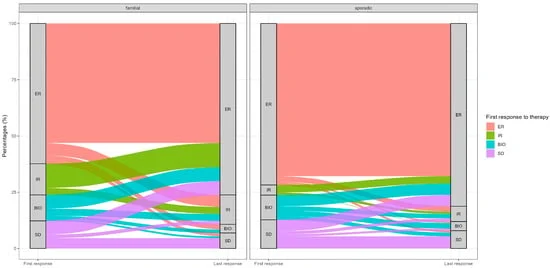
Between the first and final assessments, the researchers tracked how patients transitioned between four clinical categories: Excellent Response (ER), Indeterminate Response (IR), Biochemical Incomplete Response (BIR), and Structural Incomplete Response (SIR).
The study revealed a stark contrast in stability:
- Sporadic cases generally maintained their initial response category throughout the study period.
- Familial cases exhibited a "dynamic" pattern, frequently shifting between categories, particularly moving from an excellent response into indeterminate or biochemical incomplete states.
Supporting Data: Why Familial Status Matters
The statistical findings underscore the unique behavior of familial thyroid cancer. In a cohort of 558 patients who had initially achieved an excellent response, those with a familial history had a significantly higher risk of losing that status (14.8% in fNMTC vs. 5.5% in sNMTC).
When researchers adjusted for other prognostic factors—such as tumor stage (T1–T4), extrathyroidal extension, and multifocality—familial status remained the sole independent predictor of losing an excellent response (Odds Ratio of 3.31).
However, the data also offered a note of optimism: when patients with a non-excellent initial response were treated, the likelihood of recovering to an excellent response was the same for both familial and sporadic cases. This confirms that while the stability of remission is more fragile in familial patients, the treatability of the disease remains consistent with sporadic thyroid cancer.
Clinical Implications: A Need for "Enhanced Vigilance"
The study’s authors argue that these findings necessitate a change in clinical guidelines. Currently, patients who achieve an excellent response are often transitioned to less frequent, routine monitoring. The research suggests that for patients with a known family history, this "de-escalation" of care might be premature.
1. From "Enhanced Intervention" to "Enhanced Vigilance"
The researchers are careful to note that their findings do not support more aggressive initial surgeries or routine, heavy-handed radioiodine usage. Because structural progression is rare and similar between the two groups, aggressive upfront treatment may constitute over-treatment. Instead, they advocate for a "precision medicine" approach—keeping familial patients on a longer, more vigilant surveillance schedule to detect biochemical shifts early.
2. Refining Risk Communication
Clinicians should explicitly discuss the concept of "response fragility" with patients who have a family history of thyroid cancer. Providing patients with a clear understanding that their remission may fluctuate—not due to a recurrence of tumor mass, but due to biochemical instability—can prevent unnecessary anxiety and ensure that follow-up appointments are kept consistently.
3. Future Research Directions
The study highlights a clear gap in current knowledge: the genetic basis for this volatility. Since the study excluded patients with known hereditary syndromes (such as those associated with medullary thyroid cancer), the "familial" nature of these cases points toward as-yet-undiscovered genetic or molecular factors that influence the post-treatment behavior of non-medullary thyroid cells.

Official Responses and Expert Perspective
The study has been met with interest by the endocrine oncology community. By using the dynamic risk stratification (DRS) model rather than relying on static, binary outcomes (e.g., "recurred" vs. "did not recur"), the researchers have provided a more nuanced look at thyroid cancer survivorship.
Dr. Maria Grazia Castagna, the senior author of the paper, emphasized the importance of the study’s timing. "In the era of personalized medicine, we can no longer treat all patients with thyroid cancer the same way simply because their initial staging appears identical," she noted. The study underscores that "familial status acts as a silent risk factor," one that requires doctors to be more proactive in their long-term monitoring, even when a patient appears to be in full remission.
As the medical field continues to move toward more individualized oncology, the results of this study serve as a benchmark for how clinicians should interpret family history in thyroid care. By treating the "Excellent Response" in familial patients as a status that requires ongoing confirmation, rather than a final conclusion, medical providers can better ensure the long-term safety and well-being of their patients.
References (Summary):
- Valerio, L., Sagnella, A., Maino, F., Mattii, E., Cartocci, A., & Castagna, M.G. (2026). Familial Status Modulates the Stability of Excellent Response in Non-Medullary Thyroid Carcinoma: Implications for Tailored Surveillance. Cancers, 18(10), 1525.
- Data derived from the University of Siena Endocrine Unit cohort study, 1990–2021.
- The study was approved by the Comitato Etico Area Vasta Sud-Est (Prot. N. 10167).