On July 1, 2026, the Centers for Medicare & Medicaid Services (CMS) will embark on an unprecedented initiative in federal healthcare policy: the Medicare GLP-1 Bridge. This temporary, 18-month demonstration program is designed to address a persistent gap in coverage for millions of Americans, providing a pathway for Medicare beneficiaries to access life-altering GLP-1 medications specifically for weight management.
While the program marks a significant shift in how the federal government approaches obesity, it remains a nuanced and highly specific intervention. Operating outside the traditional Medicare Part D benefit structure, the Bridge program balances the urgent demand for modern weight-loss treatments with the fiscal realities and statutory limitations that have historically prevented Medicare from covering weight-loss drugs.
Main Facts: A New Chapter in Medicare Coverage
For years, Medicare has been legally prohibited from covering drugs used exclusively for weight loss. The GLP-1 Bridge program does not repeal this law; rather, it utilizes the federal government’s Section 402 demonstration authority. By establishing this pilot project, CMS is testing a new model to determine the impact of providing, covering, and monitoring these high-demand medications within the Medicare population.
Key Components of the Program:
- Duration: The program runs from July 2026 through December 2027.
- Eligible Medications: Coverage is restricted to three specific FDA-approved GLP-1 drugs for chronic weight management: Wegovy, Zepbound, and Foundayo.
- Cost Structure: Beneficiaries will face a flat $50 monthly copayment. Crucially, this payment does not count toward the Part D deductible or the out-of-pocket spending cap, and Low-Income Subsidy (LIS) assistance does not apply.
- Regulatory Status: Because it operates as a demonstration project, the program remains siloed from the standard Part D payment system, effectively bypassing the statutory ban while maintaining strict oversight.
Chronology: From Policy Proposal to Implementation
The road to the Bridge program has been marked by mounting pressure from patient advocacy groups and the clinical community, countered by intense federal scrutiny regarding the astronomical costs of these medications.
- Pre-2026: Persistent legislative debate and calls for Medicare to modernize its drug formulary to include anti-obesity medications (AOMs).
- July 2026: The official launch of the Medicare GLP-1 Bridge. The program opens its doors to enrollees who meet the stringent clinical and diagnostic criteria.
- July 2026 – December 2027: The 18-month demonstration period. During this time, CMS will collect data on patient adherence, health outcomes, and the overall budgetary impact on the Medicare Trust Fund.
- Post-2027: The conclusion of the demonstration. Data gathered during these 18 months will likely inform future Congressional and administrative decisions regarding the permanent inclusion of weight-loss drugs in the standard Medicare benefit.
Supporting Data: Understanding the Eligible Population
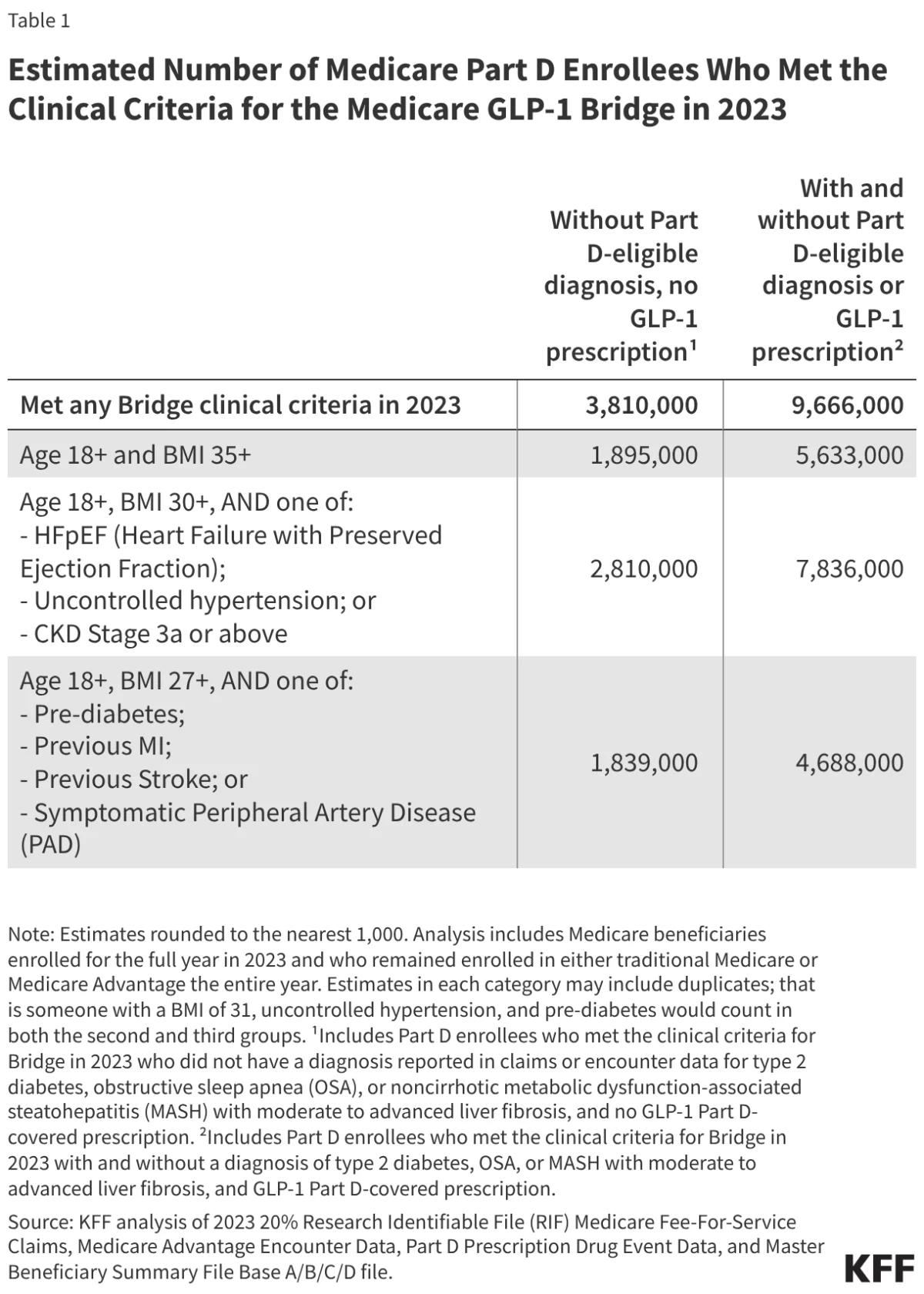
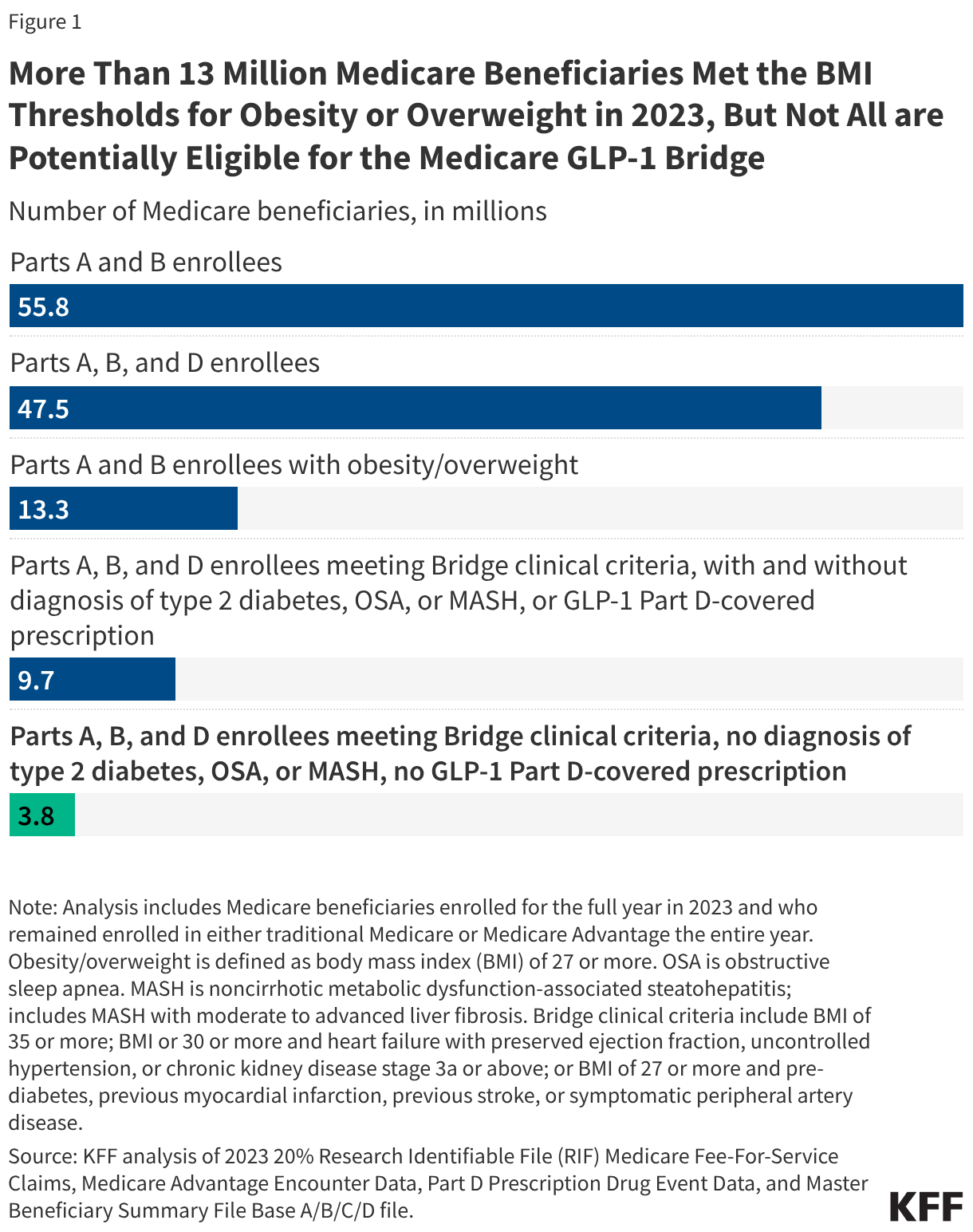
Quantifying the potential reach of this program is a complex task. According to an analysis of 2023 Medicare claims and enrollment data, approximately 13.3 million Medicare beneficiaries met the BMI threshold for obesity or overweight. However, not all of these individuals are candidates for the Bridge.
The Eligibility Filter
To ensure the program remains targeted and fiscally manageable, CMS has implemented rigorous exclusion criteria:
- Exclusion of Existing Users: Any beneficiary who already filled a prescription for a GLP-1 under their Part D plan in 2026 is ineligible.
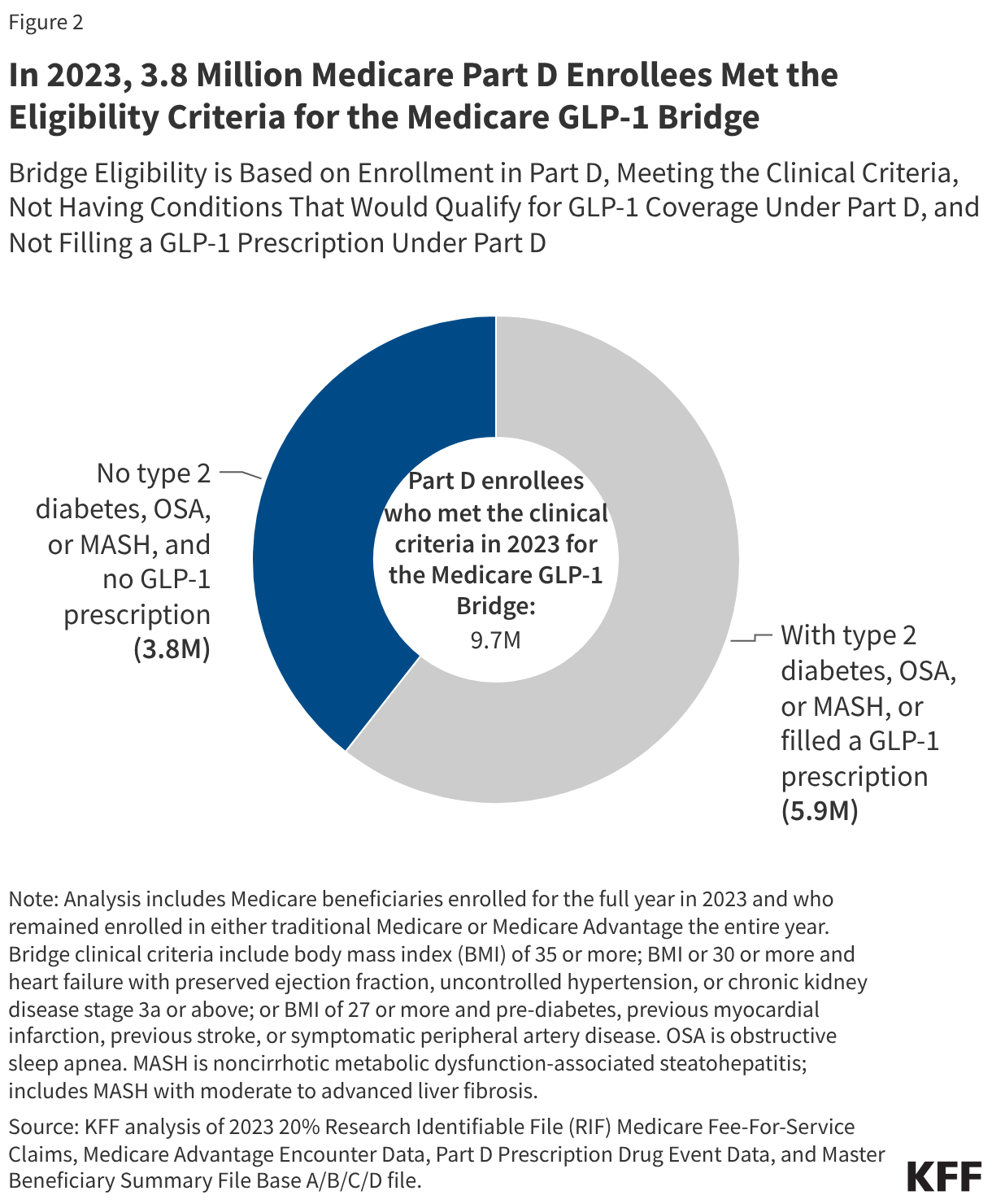
- Exclusion of Comorbidities: Individuals with type 2 diabetes, obstructive sleep apnea (OSA), or noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH) are ineligible for the Bridge. Because these conditions are already "medically accepted indications" for GLP-1s, these patients are expected to seek coverage through their standard Part D plans rather than the Bridge.
The Numbers
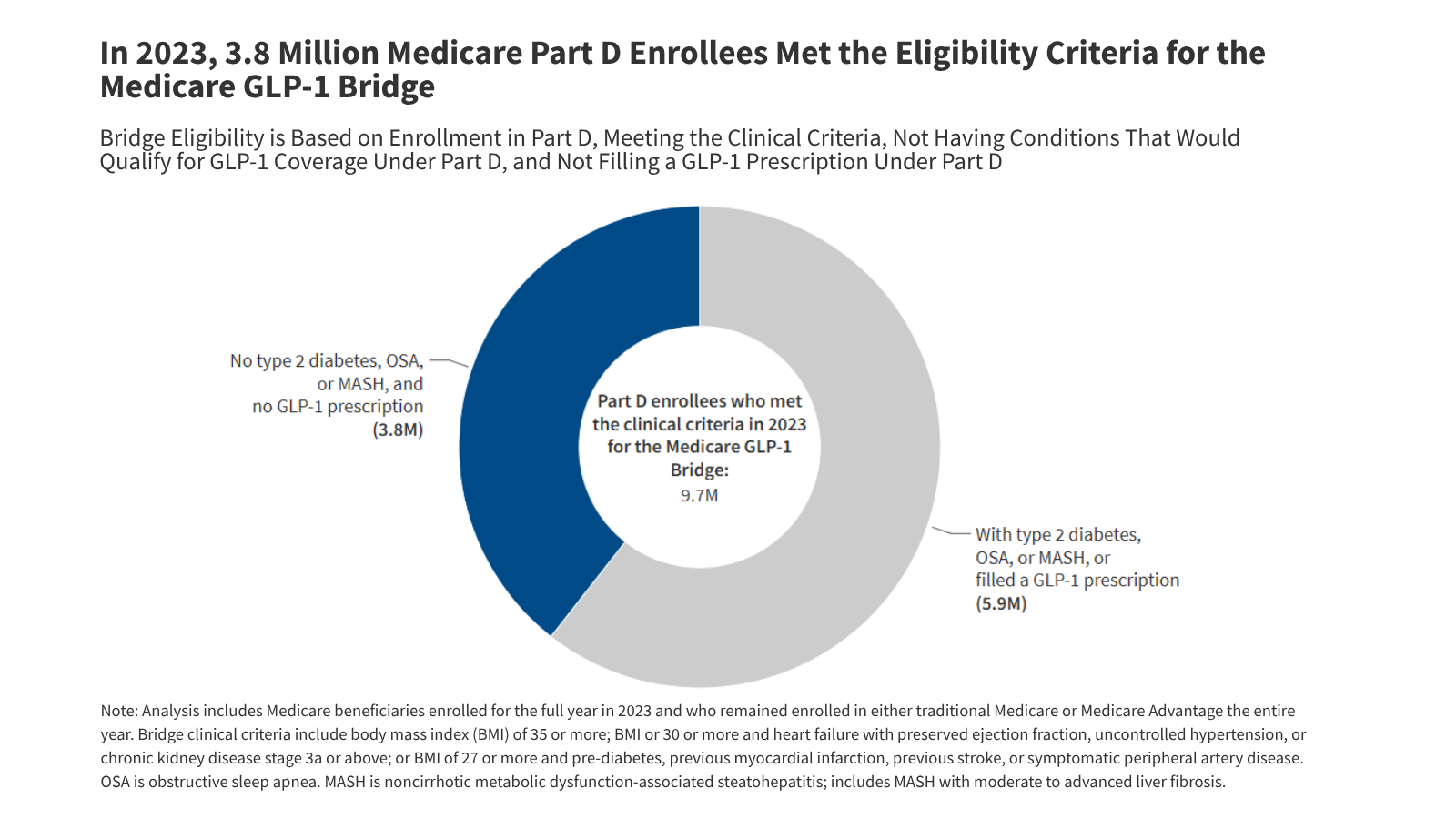
Out of 47.5 million Part D enrollees in 2023, approximately 9.7 million met the clinical criteria for weight management. Once the exclusionary filters were applied, that number dropped to 3.8 million potentially eligible beneficiaries. This represents roughly 8% of the total Part D population, highlighting that the Bridge program, while significant, is intended for a specific subset of the population that currently lacks any other access to these therapies.
Official Responses and Clinical Oversight
The implementation of the Bridge program requires a heavy administrative lift, particularly regarding the prior authorization process. Prescribing clinicians are tasked with a critical gatekeeping role. To enroll a patient, a physician must:
- Attest that the prescription is intended for weight reduction/management.
- Verify that the patient meets the specific BMI and comorbidity thresholds (e.g., BMI of 35+ or BMI of 27+ with specific cardiovascular or metabolic history).
- Formally certify that the patient does not possess any of the excluded diagnoses (Type 2 Diabetes, OSA, or MASH).
Chris Klomp, the director of Medicare at CMS, has signaled that the agency anticipates "single-digit millions" of participants. CMS remains cautious, emphasizing that the program’s success—and its potential for extension or expansion—will be heavily dependent on the clinical outcomes and the accuracy of the prior authorization attestations.
Implications: The High Cost of Access
The financial implications of the Medicare GLP-1 Bridge are substantial and represent one of the most debated aspects of the program.
Estimated Costs
The cost to the federal government depends on three volatile variables: the number of eligible participants, the rate of program adoption (take-up), and the length of adherence to the medication.
- Moderate Participation (10%–25%): If between 380,000 and 950,000 beneficiaries participate, the cost to the federal government is estimated to fall between $1.3 billion and $3.3 billion.
- High Participation (50%–75%): If the program sees widespread adoption, federal expenditures could balloon to between $6.7 billion and $10 billion.
The "Bridge" Effect
The program is aptly named. It is designed to act as a bridge—not just for patients, but for policy. By observing 18 months of real-world data, the federal government hopes to determine if the health improvements associated with weight loss (such as reduced rates of cardiovascular events, stroke, and joint surgery) will create long-term cost offsets that justify the initial investment.
However, the exclusion of those with diabetes and sleep apnea remains a point of contention. While necessary to prevent "shifting" costs from standard Part D plans to the Bridge, critics argue it creates a two-tiered system where those with the most severe weight-related comorbidities are treated under different, potentially more complex, regulatory frameworks than those who are "just" obese.
Ethical and Health Equity Concerns
From an equity perspective, the program is a double-edged sword. While it provides a $50 copayment option for a class of drugs that otherwise costs thousands of dollars per year, the administrative burden of prior authorization—and the fact that LIS cost-sharing assistance does not apply—may create hurdles for the most vulnerable beneficiaries. For low-income seniors, even a $50 monthly copayment, when multiplied by 18 months and excluding other safety-net protections, could be a financial deterrent.
Conclusion
The Medicare GLP-1 Bridge represents a bold, if limited, experiment in the evolution of American healthcare. By leveraging Section 402 demonstration authority, CMS is effectively "testing the waters" of universal obesity drug coverage.
As the program approaches its July 2026 start date, stakeholders—from pharmaceutical manufacturers to hospital administrators and patient advocates—will be watching closely. Whether this program becomes a permanent fixture of Medicare or remains a temporary footnote in the history of obesity treatment will depend entirely on the next 18 months of data. If the program successfully demonstrates that weight management leads to tangible, long-term health improvements and reduced overall spending on secondary conditions, it could pave the way for a permanent, more robust inclusion of GLP-1s in the Medicare benefit. Until then, it stands as a cautious, calculated effort to address one of the most pressing public health crises of the modern era.