As the landscape of obesity treatment undergoes a seismic shift, the U.S. government is taking a measured, experimental step into uncharted territory. A recent analysis from the Kaiser Family Foundation (KFF) sheds light on the scope and potential fiscal impact of the “Medicare GLP-1 Bridge,” a temporary federal program designed to provide coverage for weight-loss medications that have previously remained largely inaccessible to the elderly and disabled populations served by Medicare.
The program, slated to run for an 18-month duration starting July 1, 2026, and concluding in December 2027, marks a significant deviation from long-standing federal policy. By offering coverage for Wegovy, Zepbound, and Foundayo, Medicare is signaling a growing acknowledgment of obesity as a clinical priority, even as it navigates the daunting financial realities of the pharmaceutical market.
The Core Facts: What the Bridge Program Entails
The Medicare GLP-1 Bridge is not a permanent expansion of benefits, but rather a targeted, time-limited pilot. The program focuses exclusively on beneficiaries enrolled in Medicare Part D—the component of the program responsible for prescription drug coverage.
Key Program Parameters:
- Duration: The program commences on July 1, 2026, and will sunset in December 2027.
- Covered Medications: Coverage is restricted to three specific GLP-1 receptor agonists: Wegovy, Zepbound, and Foundayo.
- Eligibility Constraints: The program is not a blanket benefit. It is strictly limited to Part D enrollees who do not currently use GLP-1s for other approved indications, such as Type 2 diabetes. Furthermore, beneficiaries must not have filled a GLP-1 prescription through their Part D plan in the months leading up to the program’s launch in 2026.
- Clinical Requirements: To qualify, a beneficiary must meet specific physiological benchmarks: a Body Mass Index (BMI) of 35 or higher, or a BMI of 27 or higher when accompanied by qualifying comorbid conditions.
This narrow tailoring is a deliberate move to contain costs while providing data on the efficacy and utilization of these high-demand drugs within the Medicare population.
A Chronology of the GLP-1 Debate
To understand the significance of the Bridge program, one must examine the years of advocacy and legislative gridlock that preceded it.
2021–2023: The Rise of the GLP-1 Revolution
The surge in popularity of GLP-1 medications, initially developed for Type 2 diabetes, created a "weight-loss craze" that swept the United States. However, Medicare beneficiaries were largely left on the sidelines. Under the Medicare Prescription Drug, Improvement, and Modernization Act of 2003, Part D plans were strictly prohibited from covering drugs used for weight loss, regardless of clinical necessity.
2024: Mounting Pressure for Reform
Patient advocacy groups, along with bipartisan coalitions in Congress, began pushing for the "Treat and Reduce Obesity Act." The argument was simple: if Medicare covers the downstream consequences of obesity—such as heart disease, hypertension, and joint replacement—it should logically cover the preventive treatment of obesity itself.
2025: Fiscal Modeling and Planning
As the demand for weight-loss drugs skyrocketed, the Congressional Budget Office (CBO) and other independent researchers began modeling the immense cost of universal coverage. These projections, often reaching tens of billions of dollars annually, led the Department of Health and Human Services (HHS) to pursue a more conservative, bridge-based approach rather than a full-scale policy overhaul.
2026: The Launch
The July 2026 start date serves as a critical junction. By this time, the supply chain for GLP-1s is expected to have stabilized, and the government will have established the administrative framework required to manage the influx of claims specifically for this new coverage tier.
Supporting Data: By the Numbers
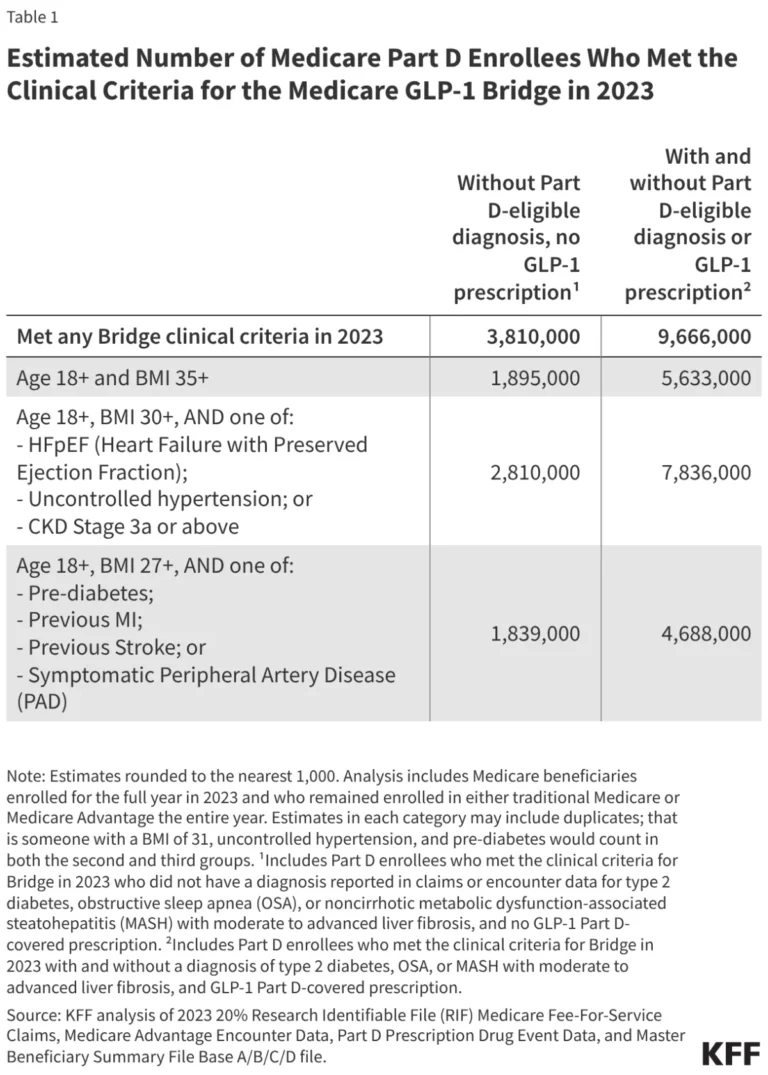
The KFF analysis provides a granular look at exactly who stands to benefit and what the cost could mean for the federal budget. While 13 million Medicare beneficiaries meet the broad BMI thresholds for obesity or overweight status, the "Bridge" program is significantly more selective.
The Eligibility Funnel:
- Broad Threshold: 13 million beneficiaries meet general BMI criteria.
- Part D Enrollment: The pool shrinks to 9.7 million when filtering for those enrolled in Part D and meeting clinical criteria.
- The "Bridge" Subset: Only 3.8 million beneficiaries meet the full, stringent requirements of the program.
Projected Fiscal Impact
The financial burden on the federal government is highly sensitive to "take-up rates"—the percentage of eligible beneficiaries who actually opt into the program.
- Low Participation (10%–25%): If a relatively small percentage of the 3.8 million eligible beneficiaries utilize the drugs, the cost is estimated at $1.3 billion to $3.3 billion over the 18-month period.
- High Participation (50%–75%): Should demand mirror the national trend in the private sector, costs could balloon to between $6.7 billion and $10 billion.
These figures are calculated based on a net monthly cost of $245 per patient, accounting for the $50 beneficiary copay. The volatility of these projections underscores why the federal government is treating this as a temporary bridge rather than a permanent entitlement.
Official Responses and Stakeholder Perspectives
The rollout of the Bridge program has elicited a complex reaction from healthcare stakeholders, ranging from cautious optimism to fiscal anxiety.
The Patient Advocacy Perspective
Organizations representing seniors and those living with chronic conditions have praised the move as a long-overdue step toward health equity. "For years, our members have been told that while obesity is a chronic disease, the most effective treatments are luxuries they cannot access," says a representative from a national patient advocacy group. "The Bridge is a start, but we must ensure that the clinical criteria don’t create barriers for those who need these medications the most."
The Fiscal Conservative Stance
Conversely, budget hawks have expressed concern about the "slippery slope." Policy analysts at the American Enterprise Institute (AEI) have warned that once a benefit is introduced—even a temporary one—it is politically difficult to revoke. "The primary concern is that this ‘bridge’ will be used as a trial run to justify permanent, massive expansion of Medicare Part D coverage, which could significantly strain the Medicare Trust Fund," one analyst noted.
Pharmaceutical Industry Reaction
The manufacturers of Wegovy, Zepbound, and Foundayo have largely remained neutral in public, focusing on the importance of "access and affordability." Behind closed doors, these companies are likely negotiating with the Centers for Medicare & Medicaid Services (CMS) regarding price points, as the government continues to exercise its new authority under the Inflation Reduction Act to negotiate drug prices.
Implications: The Future of Medicare and Obesity Care
The implementation of the Medicare GLP-1 Bridge carries profound implications for the future of American healthcare.
1. The Redefinition of "Medically Necessary"
By covering weight-loss drugs, even on a trial basis, Medicare is essentially codifying the belief that obesity is a medical condition requiring pharmaceutical intervention rather than a lifestyle issue. This shift will likely influence private insurers, who often follow Medicare’s lead in determining their own coverage tiers.
2. The Data Collection Opportunity
The 18-month duration of the program is not arbitrary; it is an analytical window. The CMS will be collecting extensive data on patient outcomes, adherence rates, and the reduction of comorbidities. If the data shows that GLP-1 usage leads to a significant decrease in hospitalizations for diabetes, stroke, and heart failure, the case for permanent, full-scale coverage will become nearly impossible for lawmakers to ignore.
3. The Burden of Cost-Sharing
The $50 monthly copay serves as a critical economic filter. For many low-income seniors on fixed incomes, this cost may still prove prohibitive, raising concerns about whether the program will effectively reach the most vulnerable populations. The success of the program will be measured not just by total spending, but by whether it reaches the diverse demographic of seniors across various socioeconomic strata.
4. Supply Chain and Logistics
The logistical challenge of providing these drugs to millions of beneficiaries cannot be understated. With current global shortages of GLP-1 medications, the sudden entry of 3.8 million potential Medicare patients could strain production capabilities. Ensuring that the supply remains consistent for those who are already on the medications will be a major test for federal regulators.
Conclusion
The Medicare GLP-1 Bridge is a landmark experiment in the evolution of federal healthcare policy. By balancing the urgent clinical needs of millions of beneficiaries against the fiscal realities of a strained Medicare budget, the government is attempting to walk a fine line.
As the program launches in July 2026, all eyes will be on the 3.8 million eligible individuals. Will they participate in the numbers projected? Will the health outcomes justify the multi-billion dollar price tag? And most importantly, will this "bridge" lead to a permanent expansion of care, or will it remain a temporary solution to a rapidly growing public health crisis?
The answers provided by this 18-month pilot will define the trajectory of obesity care in the United States for the next generation. For now, the Bridge stands as a testament to the fact that while the path toward universal access to weight-loss treatments is fraught with financial and political obstacles, the momentum is undeniably moving toward integration. As the program progresses, it will provide the definitive evidence needed to determine if the nation is ready to fully embrace the pharmaceutical management of obesity within the Medicare system.