For decades, the federal government maintained a rigid barrier between Medicaid funding and the nation’s most intensive behavioral health facilities. Known as the "IMD payment exclusion," this policy prohibited federal reimbursement for inpatient or residential care provided in "Institutions for Mental Disease" (IMDs)—facilities with more than 16 beds dedicated to psychiatric or substance use treatment. While intended to prevent the institutionalization of patients, the policy inadvertently created a funding desert for those with the most severe substance use disorders (SUDs).
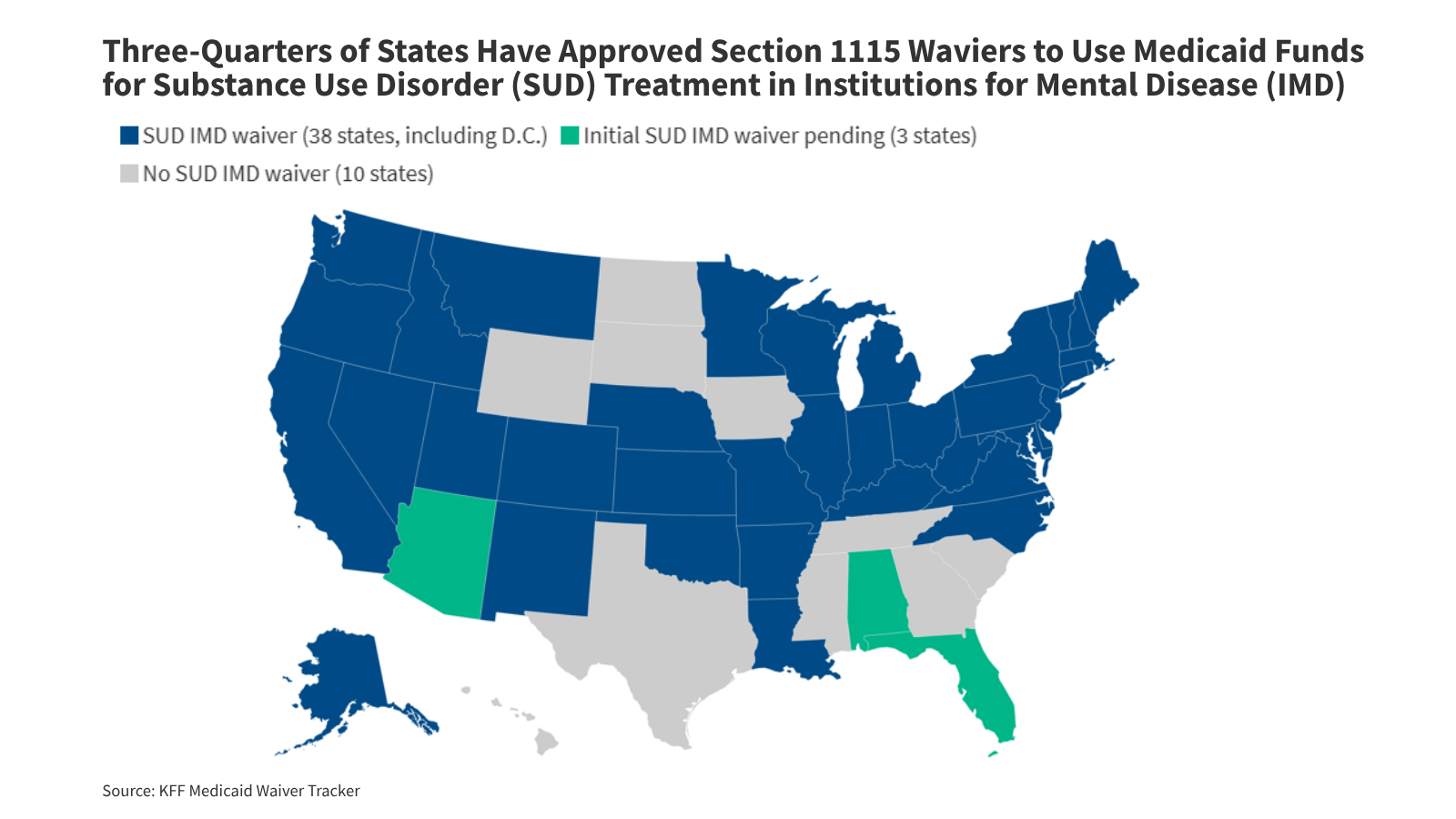
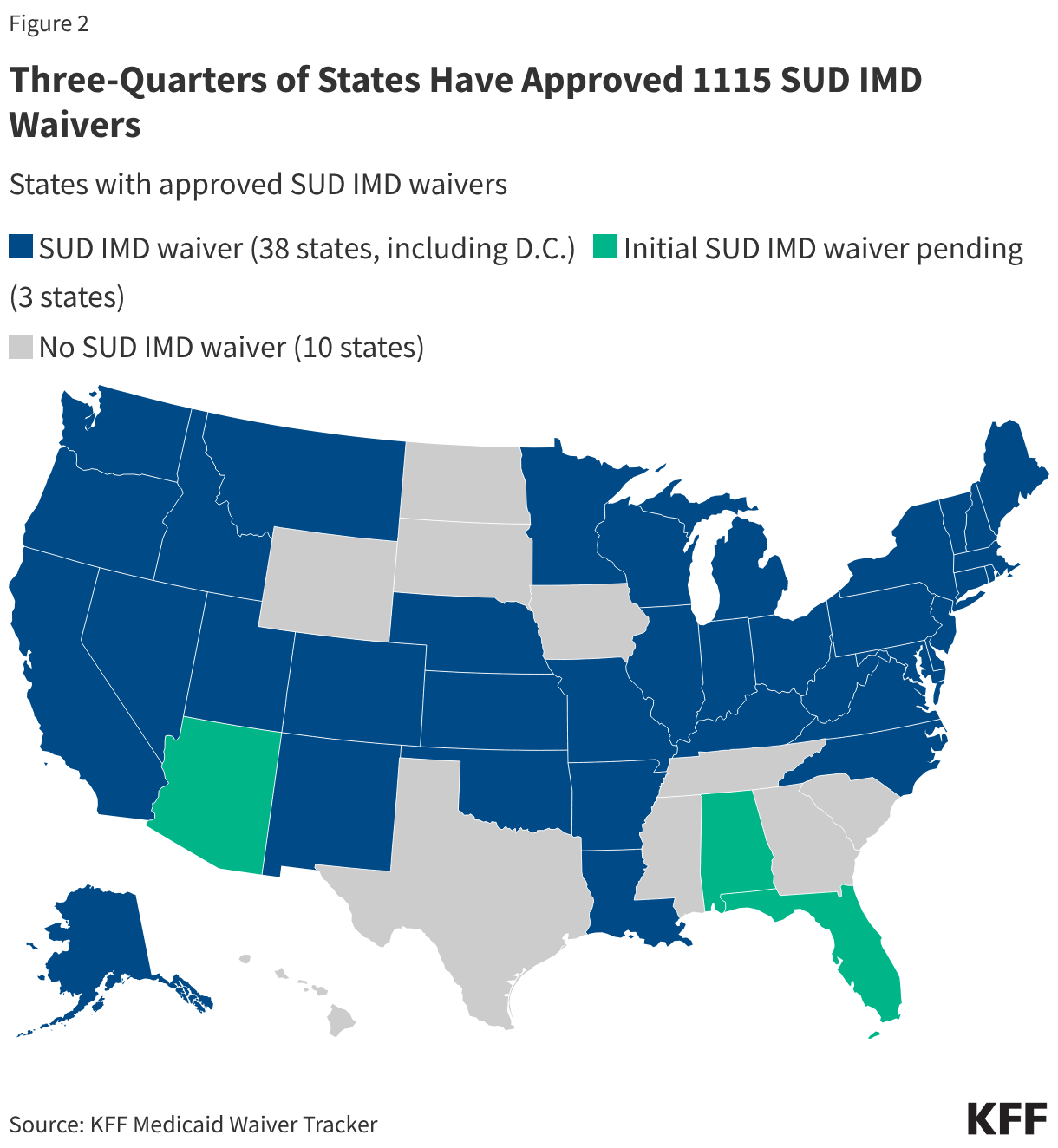
Today, that landscape is undergoing a radical transformation. Through Section 1115 demonstration waivers, 38 states have now bypassed this exclusion, securing federal matching funds to cover short-term residential and inpatient stays. As the first wave of these "SUD IMD waivers" reaches its maturity, the data reveals a complex, evolving picture of a system struggling to balance high-acuity care with the need for community-based support.
The Evolution of Federal Policy: A Chronology of Change
The journey toward modernizing Medicaid’s approach to substance use began in earnest during the height of the opioid crisis, as states struggled to find funding for the necessary surge in treatment capacity.
- 1965–2014: The Era of Exclusion. Since the inception of Medicaid, the IMD exclusion was a cornerstone of federal policy. The intent was to ensure that state governments—rather than the federal government—remained the primary financiers of inpatient mental health and substance use care.
- 2015: The Pivot. Recognizing the devastating impact of the opioid epidemic, the Centers for Medicare & Medicaid Services (CMS) issued landmark guidance allowing states to apply for Section 1115 waivers. This effectively "unlocked" federal funding for short-term stays in IMDs, provided the care was part of a larger, coordinated continuum.
- 2017: Refining the Framework. CMS updated its guidance to provide more granular expectations, emphasizing provider qualifications, the implementation of evidence-based prescribing guidelines, and the integration of Prescription Drug Monitoring Programs (PDMPs).
- 2018: The SUPPORT Act. Further cementing this shift, the federal government enacted the SUPPORT for Patients and Communities Act, creating a permanent state plan option for limited IMD coverage, which was later made permanent in the 2024 Consolidated Appropriations Act.
- 2025–2026: The Era of Summative Evaluation. As the first generation of five-year waivers concludes, states are releasing their required summative evaluations. These reports offer the first comprehensive, if preliminary, evidence on whether these waivers are actually reducing overdose deaths and improving long-term recovery outcomes.
Understanding the IMD Landscape: What is at Stake?
At its core, an IMD is an administrative designation, not necessarily a clinical one. Any hospital or residential facility with more than 16 beds primarily engaged in diagnosing or treating mental health or substance use disorders is considered an IMD.
While these facilities are vital for high-acuity, 24/7 care, they exist alongside a vast network of outpatient, crisis, and emergency services that have never been subject to the IMD exclusion. The policy tension lies in a fundamental question: Does funding large, residential institutions divert resources away from the community-based support systems that are essential for long-term recovery?
Critics of the expansion argue that by funneling money into "brick and mortar" institutions, states may neglect the outpatient infrastructure required for sustainable, independent living. Proponents, however, point to the clinical reality that for individuals in the throes of severe addiction, residential stabilization is often the only way to prevent immediate mortality.
Data-Driven Insights: Findings from the Front Lines
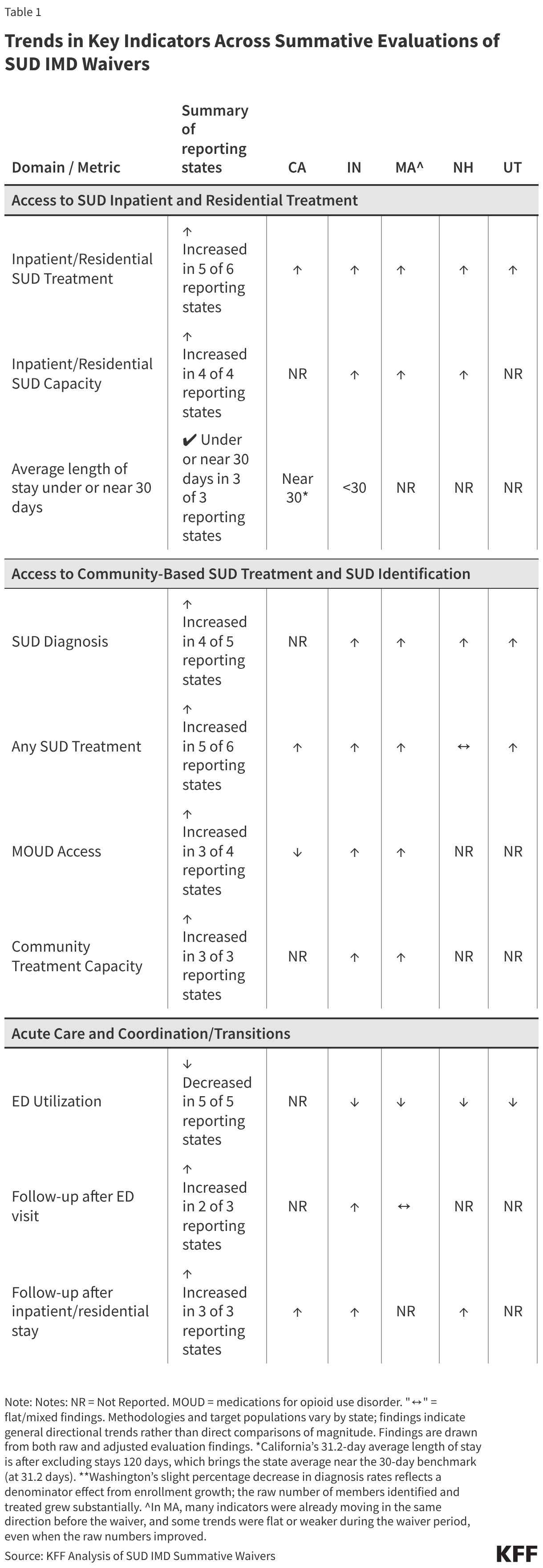
The six states that have released their summative evaluations—California, Indiana, New Hampshire, Utah, Washington, and Massachusetts—provide a high-level view of the waiver’s impact. While the data is not universally causal, it offers "directional signals" for policymakers.
Expanded Access and Utilization
Across all six states, there was a measurable increase in the utilization of inpatient and residential SUD services. This is not unexpected; by removing the financial barrier to using IMD beds, Medicaid programs effectively increased the number of available treatment slots. Data indicates that states have also seen an uptick in the number of individuals diagnosed with SUDs, suggesting that the expanded coverage is helping to identify and engage patients who were previously lost to the system.
The Community Capacity Dilemma
One of the most critical goals of the 1115 waivers was to strengthen the entire continuum of care, not just inpatient stays. Results are mixed here. While some states reported an increase in the availability of medications for opioid use disorder (MOUD)—such as methadone and buprenorphine—the expansion of community-based outpatient services remains inconsistent. The "hand-off" from a secure residential facility to a community provider remains a point of systemic failure in many jurisdictions.
Trends in Emergency Department (ED) Usage
A significant goal for these waivers was the reduction of "avoidable" acute care usage. Encouragingly, most evaluations pointed to a decline in SUD-related ED visits. By providing a stable residential alternative to the hospital emergency room, these waivers appear to be alleviating some of the pressure on the traditional, and often more expensive, emergency medical system.
Official Responses and Policy Perspectives
The federal government, under recent administrations, has maintained a consistent focus on the "continuum of care" model. CMS has repeatedly stressed that while residential IMD care is a vital tool, it must not act as a silo.
However, external policy shifts are creating new pressures. The 2025 Reconciliation Law, for instance, introduced new restrictions in Medicaid financing that may threaten the incremental expansions of mental health and SUD benefits achieved over the last decade. Furthermore, a recent Department of Justice opinion regarding the intersection of homelessness and substance use may force states to rethink how they deliver involuntary or semi-voluntary care.
In interviews, state-level health directors have expressed a dual sentiment: they are grateful for the flexibility the 1115 waivers provide, but they are increasingly concerned about the administrative burden of managing these programs. "The paperwork required to maintain compliance with these waivers is significant," noted one state health official. "We are effectively operating two different systems of care—one that is highly regulated for IMD stays and one that is more flexible but under-resourced."
Barriers to Success: What the Evaluations Missed
While the quantitative data tracks successes in bed capacity and diagnosis rates, the qualitative findings from stakeholder interviews highlight the "human" side of the policy failure:
- The Workforce Crisis: Across all reporting states, the primary bottleneck is not money or beds—it is people. A chronic shortage of licensed addiction counselors, psychiatrists, and nursing staff limits the effectiveness of any facility, regardless of its funding status.
- Fragmented Care Coordination: In states where Medicaid physical health and behavioral health benefits are split across different managed care plans, the "hand-off" becomes a "black hole." Patients frequently lose access to their treatment teams when they transition from an IMD back to their home environment.
- Administrative Burdens: The complexity of prior authorization and billing processes often discourages smaller providers from participating. This creates a market where only large, hospital-affiliated organizations can afford the administrative cost of treating Medicaid patients, potentially reducing the diversity of available care.
- The Housing Paradox: Perhaps the most poignant finding across all six state evaluations is the role of housing. Many providers noted that discharging a patient from a secure residential facility back into a state of homelessness or housing instability leads to an almost immediate "downward spiral." Without a stable place to sleep, the clinical gains of the residential stay are rapidly eroded.
Implications for the Future of Addiction Care
As more states complete their evaluations, the national conversation is moving toward a more nuanced understanding of "what works." The era of simply removing the IMD exclusion is giving way to an era of integration.
The future of Medicaid SUD policy will likely focus on three pillars:
- Workforce Development: Policy initiatives that incentivize the training and retention of the behavioral health workforce are likely to become as important as the funding of the facilities themselves.
- Housing-First Models: Evaluations make it clear that clinical treatment cannot exist in a vacuum. Integrating housing support into the Medicaid benefit package for individuals in recovery is no longer seen as an optional extra, but as a clinical necessity.
- Standardization of Care Transitions: Federal and state regulators are under increasing pressure to mandate stricter, more standardized protocols for discharging patients from IMDs. The "black hole" of coordination between hospital and home must be replaced by a seamless "warm hand-off" that involves peer support specialists and community-based primary care.
Ultimately, the 1115 SUD IMD waivers have proven that money can increase capacity. The next, and far more difficult, challenge is to ensure that this capacity is used to build a robust, sustainable, and community-centric system of care that addresses not just the addiction, but the person. As the evidence base grows, the focus must shift from merely providing a bed to ensuring that the patient has a path forward after the doors of that facility close.