By Medical Science Correspondent
Intraductal papillary mucinous neoplasms (IPMN) represent a complex challenge in modern gastroenterology. As cystic lesions of the pancreas with significant malignant potential, their management requires a delicate balance between surgical intervention and conservative surveillance. A recent multicenter study published in the journal Diagnostics (May 2026) has shed new light on the utility of peroral pancreatoscopy (POPS) using the 9-Fr eyeMAX system, offering a potential breakthrough in how surgeons plan complex pancreatic procedures.
The Challenge of MD/Mixed-IPMN
Intraductal papillary mucinous neoplasms, particularly those involving the main pancreatic duct (MD-IPMN) or mixed-type variants, are known to harbor a higher risk of invasive carcinoma compared to their branch-duct counterparts. Current international guidelines strongly recommend surgical resection for patients exhibiting "high-risk stigmata" (HRS).

However, the primary hurdle for surgeons remains the preoperative determination of the exact longitudinal extent of the tumor. Because IPMNs often manifest as diffuse, microscopic spread along the main pancreatic duct, surgeons frequently face the dilemma of choosing between a localized resection or a total pancreatectomy. While standard imaging modalities like CT and MRI are essential for initial diagnosis, they often fail to capture the subtle, high-resolution details required to map the exact boundary of a tumor.
Chronology of the Multicenter Study
The retrospective analysis, led by Dr. Haruo Miwa and his team at Yokohama City University Medical Center, evaluated 20 consecutive patients treated between May 2023 and September 2025.
- May 2023: The study period commenced, focusing on patients with MD/mixed-IPMN who required further evaluation beyond standard imaging.
- January 2024: The study received official Institutional Review Board (IRB) approval (Approval No. F220300060).
- March 2026: Final data collection was completed, and the manuscript was submitted for peer review.
- May 2026: Following a successful peer-review process and revisions, the study was published, documenting a technical success rate of 95% for the 9-Fr eyeMAX procedure.
Technical Innovation: The 9-Fr EyeMAX
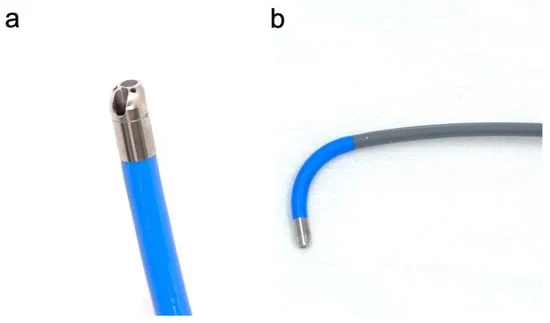
The study centered on the use of the 9-Fr eyeMAX (Micro-Tech, Nanjing, China), a next-generation slim cholangioscope. With an outer diameter of only 3.2 mm, the device features a four-way tip deflection system and an independent irrigation channel.
These design specifications are critical. In the narrow, often tortuous anatomy of the pancreatic duct, conventional endoscopes are frequently too rigid or large, leading to increased risk of post-ERCP pancreatitis. The eyeMAX’s ability to maintain high-quality digital imaging while navigating acute angulations—without requiring heavy saline irrigation—marks a significant step forward in procedural safety.
Supporting Data: Findings and Outcomes
The clinical findings presented in the study offer a granular view of the procedure’s performance:
- Diagnostic Precision: In 85% of cases (17 out of 20), POPS successfully identified mural nodules. Notably, in five patients who had appeared "clean" on endoscopic ultrasonography (EUS), the eyeMAX successfully detected occult mural nodules.
- Safety Profile: The primary fear with pancreatoscopy is pancreatitis. In this cohort, the incidence was remarkably low, with only one instance of mild post-ERCP pancreatitis (5%), which was managed conservatively.
- Surgical Impact: Of the 12 patients who underwent surgery, the POPS findings directly informed the surgical strategy. For instance, in patients where EUS suggested localized disease but POPS revealed diffuse involvement, surgeons were able to reconsider the extent of the resection, avoiding both undertreatment and the morbidity of unnecessary total pancreatectomy.
Official Perspectives and Diagnostic Limitations
Despite the technical success, the research team emphasized a note of caution regarding biopsy reliability. The study found that the concordance rate between POPS-guided biopsy and final surgical pathology was only 45%.

Dr. Miwa’s team noted that this limitation is inherent to the biopsy process: "The biopsy specimens obtained are often small, and the histological heterogeneity of IPMN means that the most aggressive component of the lesion may be missed." Consequently, the authors conclude that POPS-guided biopsy should not be treated as a standalone "gold standard" for grading dysplasia or excluding malignancy. Instead, it serves as an adjunctive, supportive tool.
Implications for Future Surgical Planning
The implications of this research are twofold. First, it validates the 9-Fr eyeMAX as a feasible, safe, and effective tool for visual mapping of the pancreatic duct, providing surgeons with a "look inside" that MRI and CT cannot replicate. Second, it shifts the expectation of what pancreatoscopy can achieve.
Instead of relying on the biopsy as the final word, clinicians are encouraged to use POPS as a navigational aid to understand the tumor’s spread. This allows for more personalized surgical planning—a concept that is becoming increasingly vital in oncology. By visualizing the "real-time" extent of a lesion, surgeons can make more informed decisions about whether to perform a distal pancreatectomy, a pancreatoduodenectomy, or a more extended resection.

Conclusion and Future Directions
The 2026 study serves as a foundational "hypothesis-generating" document. While the small sample size precludes a definitive change in international guidelines, the high technical success rate and the ability to detect nodules missed by EUS suggest that the 9-Fr eyeMAX will likely see increased utilization in tertiary referral centers.
As future research moves toward larger, prospective cohorts, the focus will likely remain on refining the biopsy technique and further clarifying which patients stand to gain the most from this invasive but highly informative procedure. For now, the integration of POPS into the preoperative workup for MD/mixed-IPMN represents a sophisticated refinement in the effort to provide precise, minimally invasive, and effective surgical care for patients with pancreatic neoplasms.
Summary of Key Findings
| Metric | Result |
|---|---|
| Technical Success Rate | 95% |
| Mural Nodule Detection | 85% |
| Mild Pancreatitis Rate | 5% |
| Biopsy-Pathology Concordance | 45% |
| Primary Utility | Adjunctive visual mapping for surgical planning |
Disclaimer: This article is based on the published research in Diagnostics (2026, 16, 1443). Clinical decisions regarding pancreatic surgery should always be made in consultation with specialized multidisciplinary oncology teams.