The landscape of American public health coverage is bracing for a seismic shift. Under the provisions of the 2025 federal budget reconciliation law, the Medicaid program—a bedrock of the safety net for millions of low-income Americans—will undergo its most significant transformation since the inception of the Affordable Care Act (ACA). For the first time in the program’s history, the federal government will mandate that states impose cost-sharing requirements on specific adult populations enrolled through the ACA’s Medicaid expansion.
This legislative pivot moves away from the historical norm, where cost sharing was largely a state-level option, toward a more rigid, federally directed framework. As the October 2028 implementation deadline approaches, policymakers, healthcare providers, and patient advocates are weighing the potential consequences: while proponents argue these measures promote personal responsibility and fiscal sustainability, researchers warn of significant barriers to care, increased financial strain on vulnerable households, and potentially poorer health outcomes.
A Historical Shift: From State Flexibility to Federal Mandates
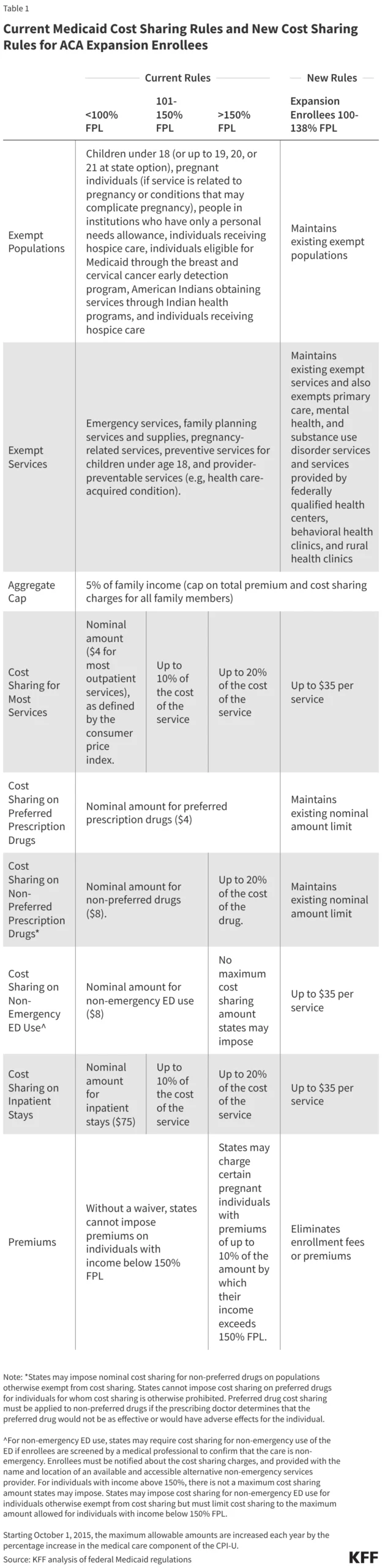
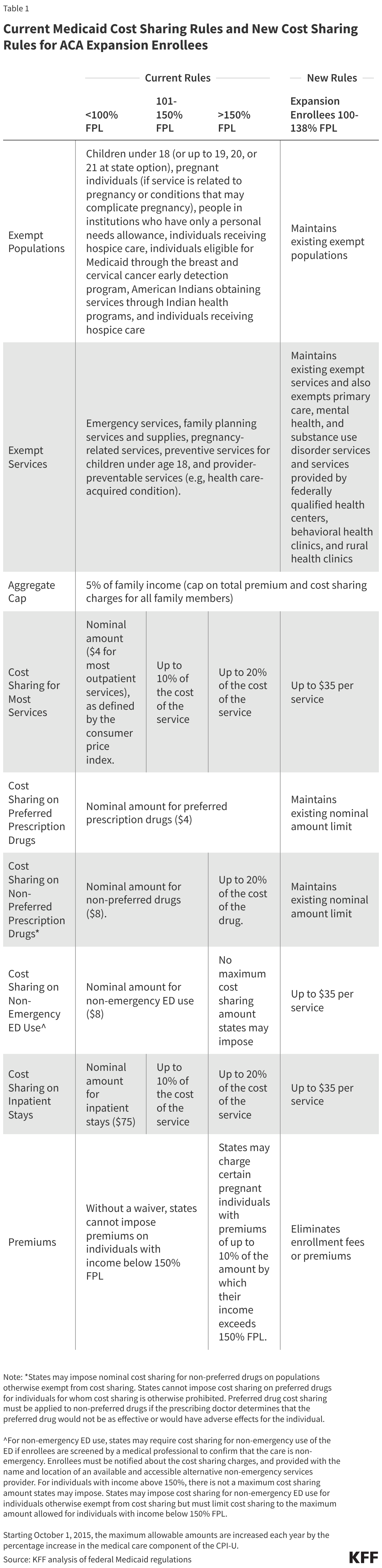
Historically, Medicaid was designed with protections to ensure that low-income enrollees were not deterred from seeking necessary care due to prohibitive costs. While federal regulations have long permitted states to charge nominal copayments or premiums, these policies were strictly optional. States could choose to implement them, provided they stayed within "nominal" limits designed to protect those living below the Federal Poverty Level (FPL).
Under existing rules, total out-of-pocket expenses for a Medicaid household are capped at 5% of their quarterly or monthly income. Furthermore, states have been required to establish administrative mechanisms—independent of the enrollee’s own record-keeping—to track these costs and trigger an automatic stop once the threshold is met.
The 2025 reconciliation law fundamentally alters this paradigm. By requiring states to impose cost-sharing on adults earning between 100% and 138% of the FPL, the federal government is shifting the program’s philosophy. No longer is the focus purely on accessibility; it is now explicitly coupled with a requirement for financial participation from the enrollee.
Chronology of Implementation and Regulatory Evolution
The rollout of these changes is structured to give states time to adapt, though the timeline remains aggressive given the complexity of Medicaid administration.
- Pre-2025 Baseline: Cost sharing remained an optional state-level policy. Nineteen states currently choose to impose some form of cost sharing on expansion adults, though the structure varies wildly—from states that only charge for prescription drugs to those with complex copayment schedules for hospital visits.
- The 2025 Reconciliation Law: The legislation was signed into law, introducing mandatory cost-sharing requirements for expansion adults (100–138% FPL) and establishing new eligibility criteria, including more frequent redetermination cycles (every six months) and work requirements.
- July 1, 2027: States like North Carolina have already begun positioning their internal policies to align with the new federal ceiling, setting copayments at the maximum allowable limits to prepare for the transition.
- October 1, 2028: The federal mandate takes full effect. States will be required to impose cost-sharing of up to $35 per service for the specified expansion population.
Supporting Data: The Current Landscape of State-Level Costs
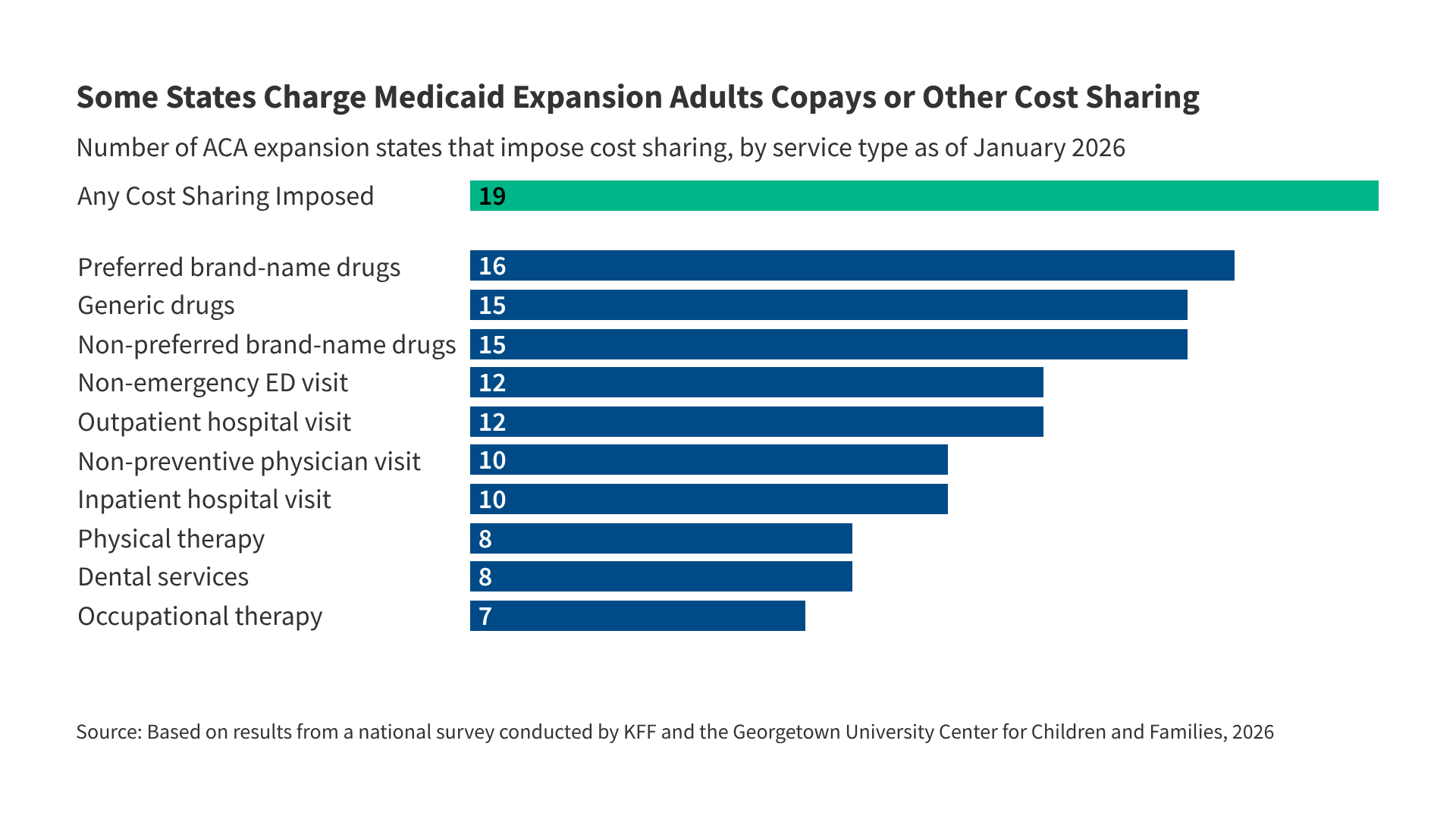
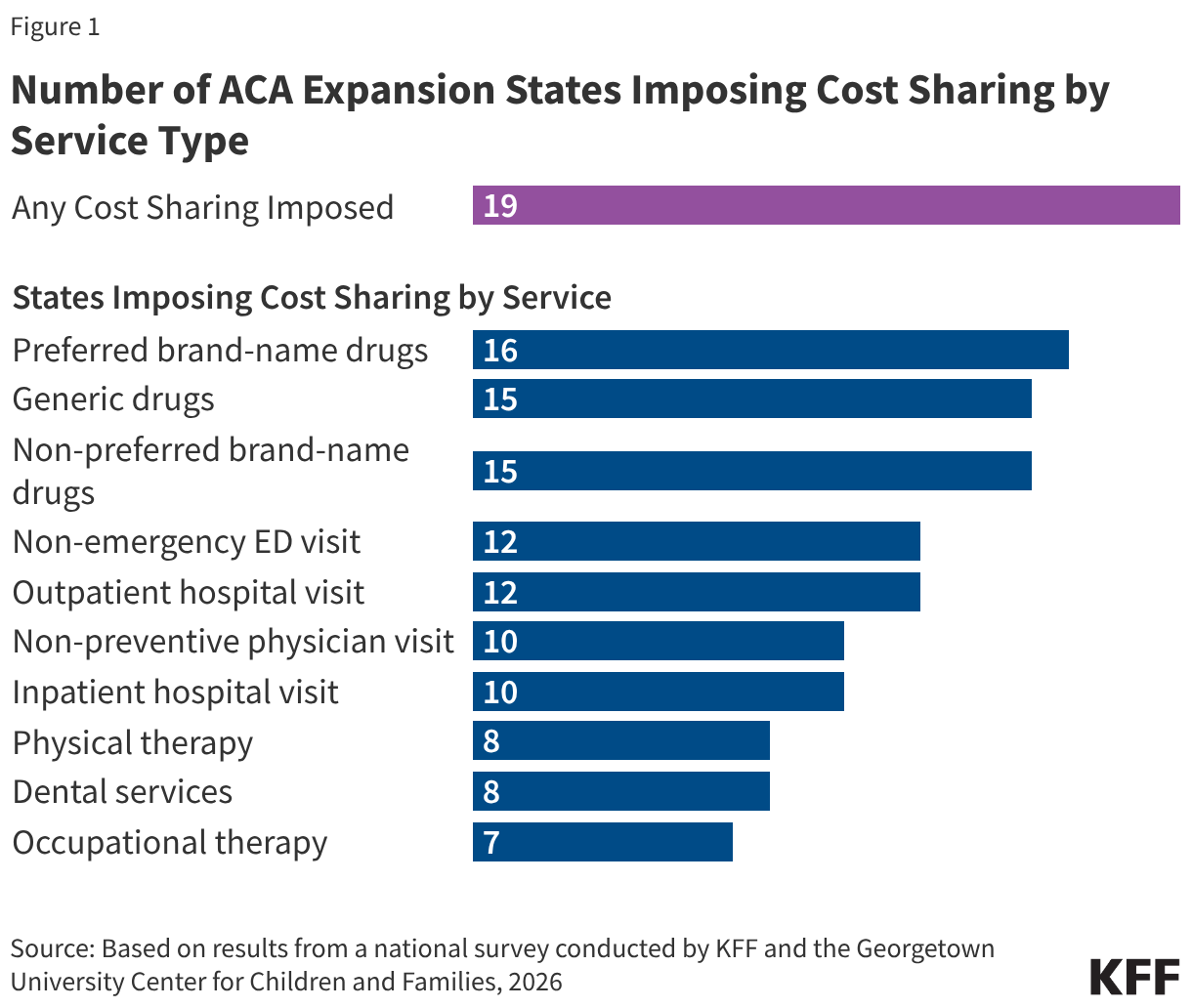
As of January 2026, the variation in state Medicaid programs provides a preview of the challenges ahead. Data collected through the KFF Medicaid Eligibility, Enrollment, and Renewal Policies Annual Survey highlights that 19 states currently charge cost-sharing for expansion adults.
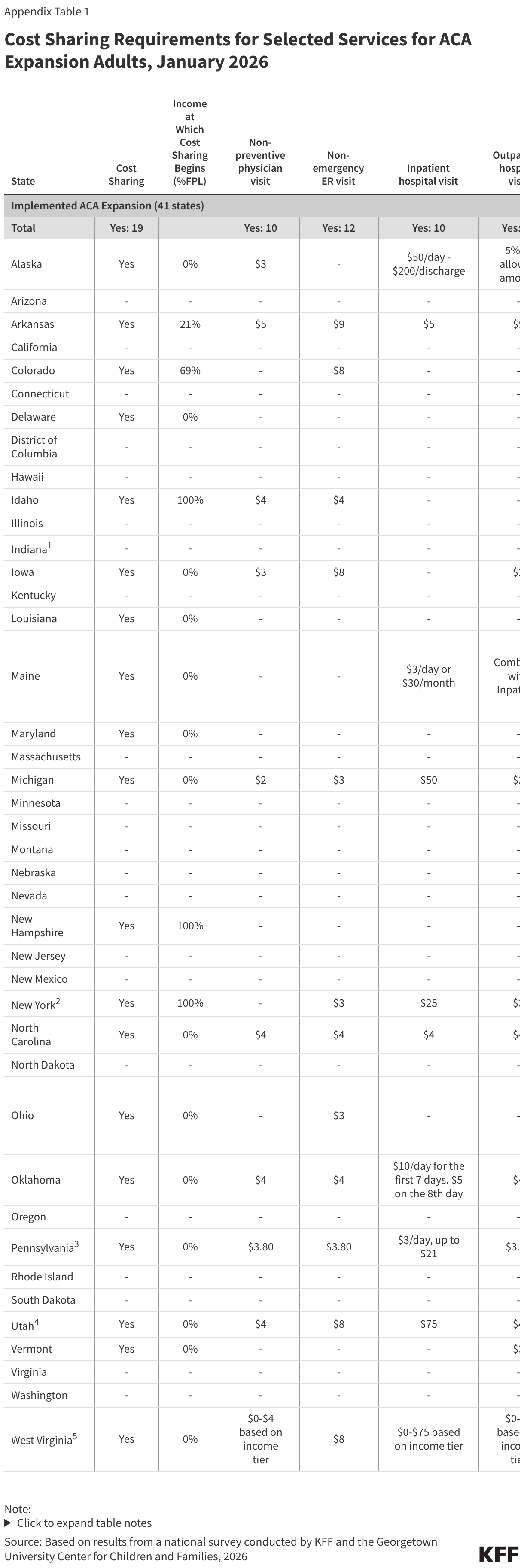
Of these, 14 states impose costs regardless of the enrollee’s income level, while others target specific income brackets. Prescription drugs are the most common service subject to fees, with 16 states charging for preferred brand-name drugs and 15 for generics.
However, the "nominal" nature of these fees is relative. While many states keep charges under $10, some have utilized their current flexibility to charge significantly higher amounts for inpatient care. For instance, Alaska, Michigan, Utah, and West Virginia currently charge more than $35 for hospital stays. These states face a significant regulatory hurdle: they must now reconcile their existing, higher cost-sharing models with the specific federal mandate of $35, potentially requiring a downward adjustment in some areas and an upward standardization in others.
The Financial and Clinical Implications for Enrollees
The primary concern among healthcare analysts is the "chilling effect" that cost-sharing has on the utilization of essential services. A robust body of literature consistently indicates that even small, out-of-pocket costs can deter low-income patients from seeking care.
Barriers to Essential Care
Evidence suggests that when cost-sharing is introduced, the most immediate casualty is often preventative care or the management of chronic conditions. Research has shown that even nominal fees reduce the utilization of medications and behavioral health services, particularly for individuals struggling with substance use disorders (SUDs). When patients delay or forgo these services, they often end up in more expensive, emergent settings—such as the emergency department—eventually driving up the total cost of care for the state.
The Disproportionate Burden on the Vulnerable
The financial impact is not distributed equally. KFF analysis reveals that the average Medicaid expansion enrollee, if faced with a $35 charge on all non-exempt services, could face annual out-of-pocket costs as high as $542. For a family living near the poverty line, this represents a significant portion of their disposable income.
Furthermore, the burden is greatest for those who need the system the most. Data suggests that:
- Older Enrollees: Those who are older, and thus more likely to have multiple chronic conditions, could face costs twice as high as their younger, healthier counterparts.
- Chronic Illness: Individuals managing multiple physical or behavioral health conditions could pay up to five times more in cost-sharing than those without such conditions.
This creates a "sickness tax," where the individuals with the least financial resilience are forced to bear the highest costs for the essential services required to maintain their health.
Official Responses and Policy Perspectives
The policy shift has drawn starkly different reactions from across the political spectrum.
Proponents of the Law: Supporters, including many who advocated for the 2025 reconciliation law, argue that these measures are essential for the long-term sustainability of the Medicaid program. They contend that requiring a nominal "skin in the game" encourages enrollees to be more judicious in their use of healthcare services, potentially reducing waste and encouraging personal accountability. From this perspective, the $35 cap is a reasonable compromise that ensures patients have access to care while preventing the system from becoming a "blank check."
Critics and Healthcare Advocates: Conversely, public health experts and patient advocacy groups argue that the move is fundamentally misguided. They point to the well-documented link between cost-sharing and increased mortality rates in low-income populations. These critics argue that "utilization" is not necessarily "waste"; often, the care that is deterred by cost-sharing is the exact type of care that keeps chronic conditions from spiraling into life-threatening emergencies. Many health departments are expressing concern that the administrative burden of tracking these payments, coupled with the new six-month redetermination requirements, will lead to a "churn" in enrollment—where eligible people lose coverage simply because they cannot navigate the increasingly complex bureaucratic hurdles.
Looking Ahead: The Challenges of 2028
As the October 2028 deadline looms, the focus turns to the Centers for Medicare & Medicaid Services (CMS). Guidance is expected to clarify the extent of state flexibility. Can states choose which services require the $35 fee, or is it a blanket mandate? How will the tracking systems be standardized across state lines?
The 2025 reconciliation law represents a bold experiment in social policy. It attempts to balance the fiscal pressures facing state budgets with the federal commitment to providing a safety net. However, as the evidence clearly shows, the intersection of poverty and healthcare is delicate. By introducing mandatory costs into a system designed to mitigate them, the federal government is initiating a high-stakes transition. Whether this leads to the intended fiscal efficiency or to a decline in public health metrics will depend entirely on how effectively states implement these mandates—and whether the administrative safety nets are strong enough to protect the most vulnerable from being priced out of their own health.