By Policy Analysis Desk
Updated June 17, 2025
A looming legislative battle in Washington threatens to reshape the landscape of American healthcare for the most vulnerable. At the center of this controversy is the "One Big Beautiful Bill Act," a reconciliation package passed by the House of Representatives on May 22, 2025. While framed as a fiscal measure to extend expiring tax cuts, the legislation proposes a fundamental shift in how the federal government approaches Medicaid, specifically targeting the administrative rules that govern enrollment and retention.
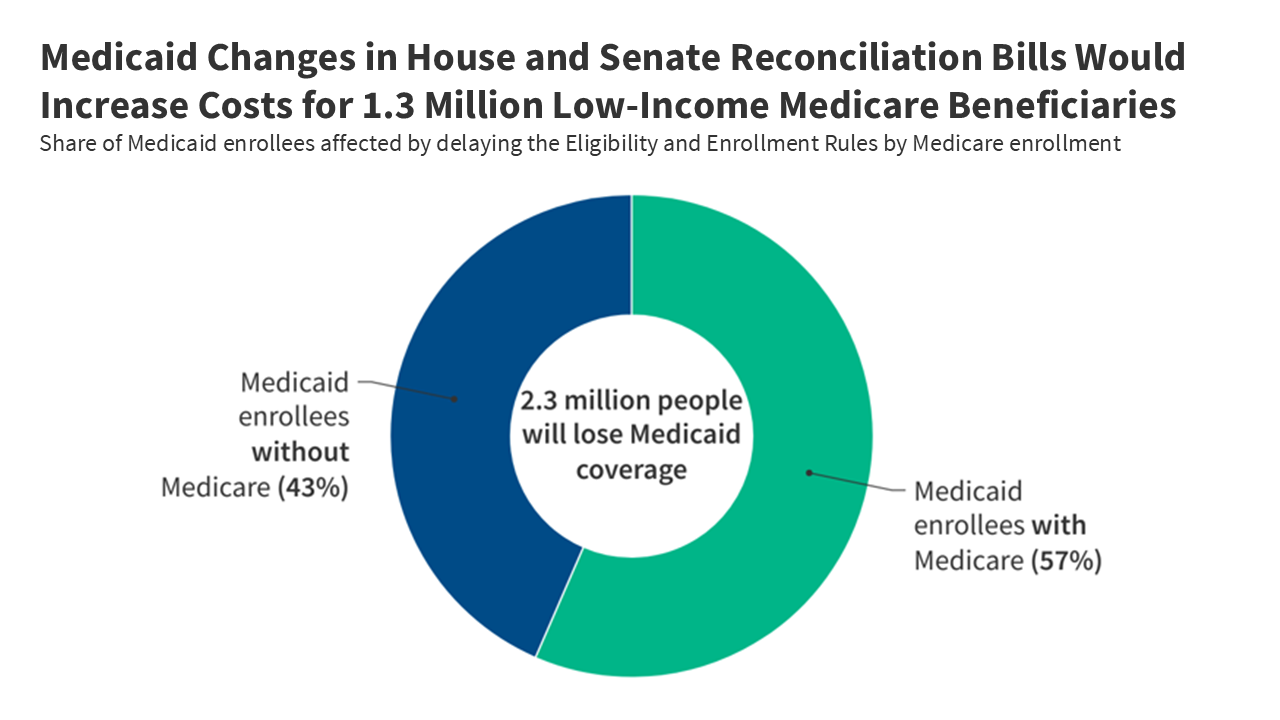
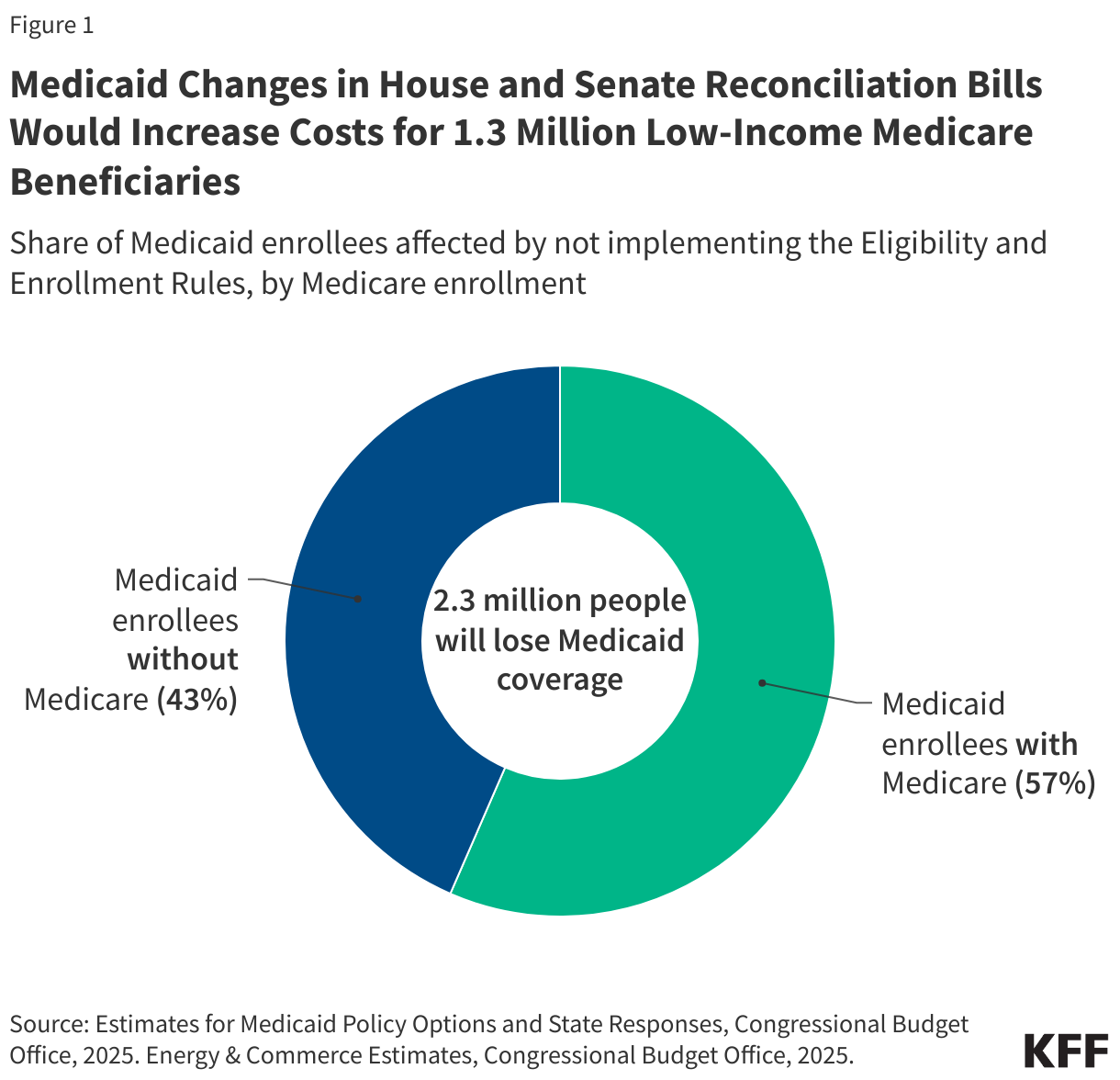
According to the Congressional Budget Office (CBO), the implications of this bill are profound. If enacted, the legislation would strip $793 billion in federal Medicaid spending over the next decade. More alarmingly, the CBO projects that by 2034, approximately 10.3 million fewer people will be enrolled in Medicaid than under current projections. Among those most severely affected are 1.3 million low-income Medicare beneficiaries—individuals who rely on the synergy between Medicaid and Medicare to afford basic medical care.
The Chronology of Legislative Action
The legislative trajectory of these cuts has been swift and contentious. Following months of debate regarding the federal deficit and the sunsetting of key tax provisions, House leadership introduced the One Big Beautiful Bill Act as a primary vehicle for fiscal consolidation.
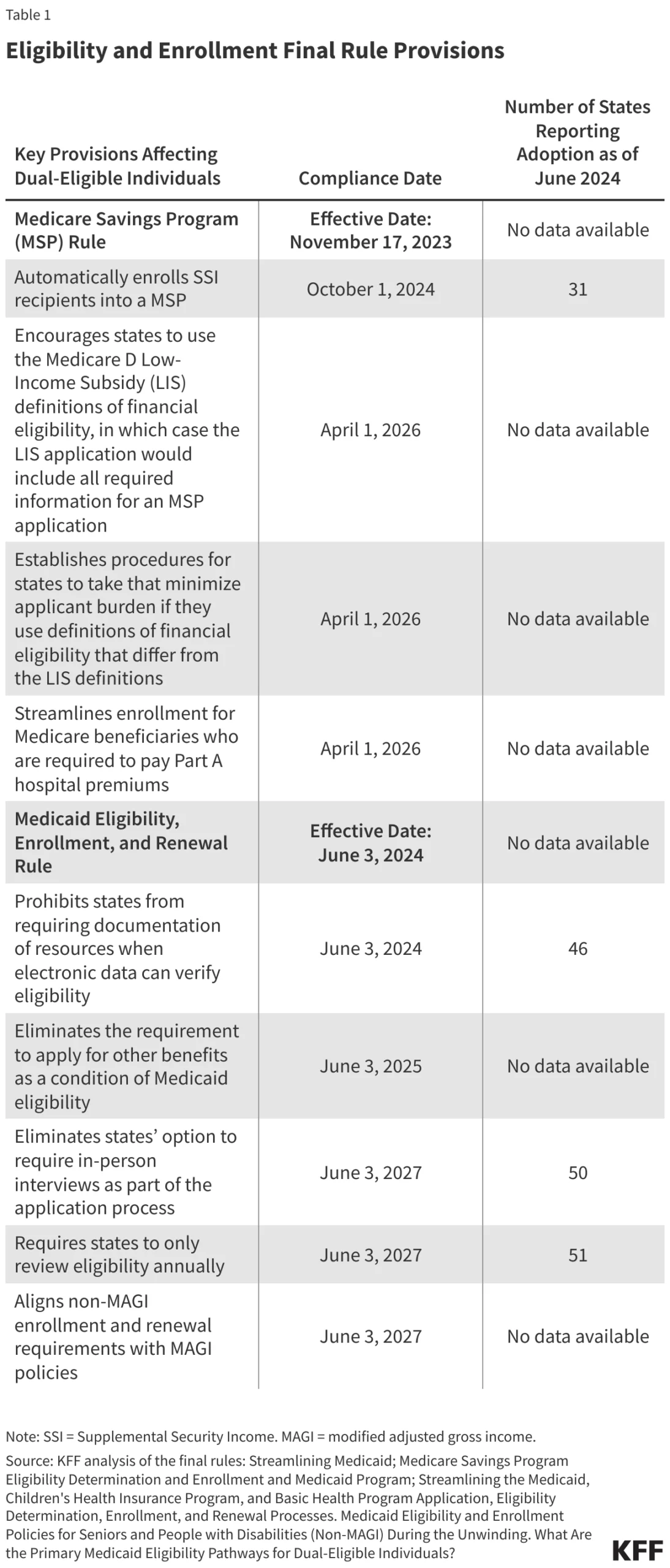
- May 22, 2025: The House of Representatives passes the reconciliation bill, signaling a major pivot in Medicaid policy. The bill specifically mandates a delay in the implementation of two Biden-era administrative rules until 2035.
- Early June 2025: Senate committees began reviewing their own version of the reconciliation language. In a significant escalation, the Senate’s draft goes beyond the House’s temporary moratorium, proposing to outright prohibit the implementation of these rules permanently.
- June 17, 2025: Following the passage of final legislative language, it becomes clear that while some concessions were made to shield certain groups, the primary mechanism of the bill remains intact, though the total number of affected low-income beneficiaries may be slightly lower than initial CBO estimates suggested.
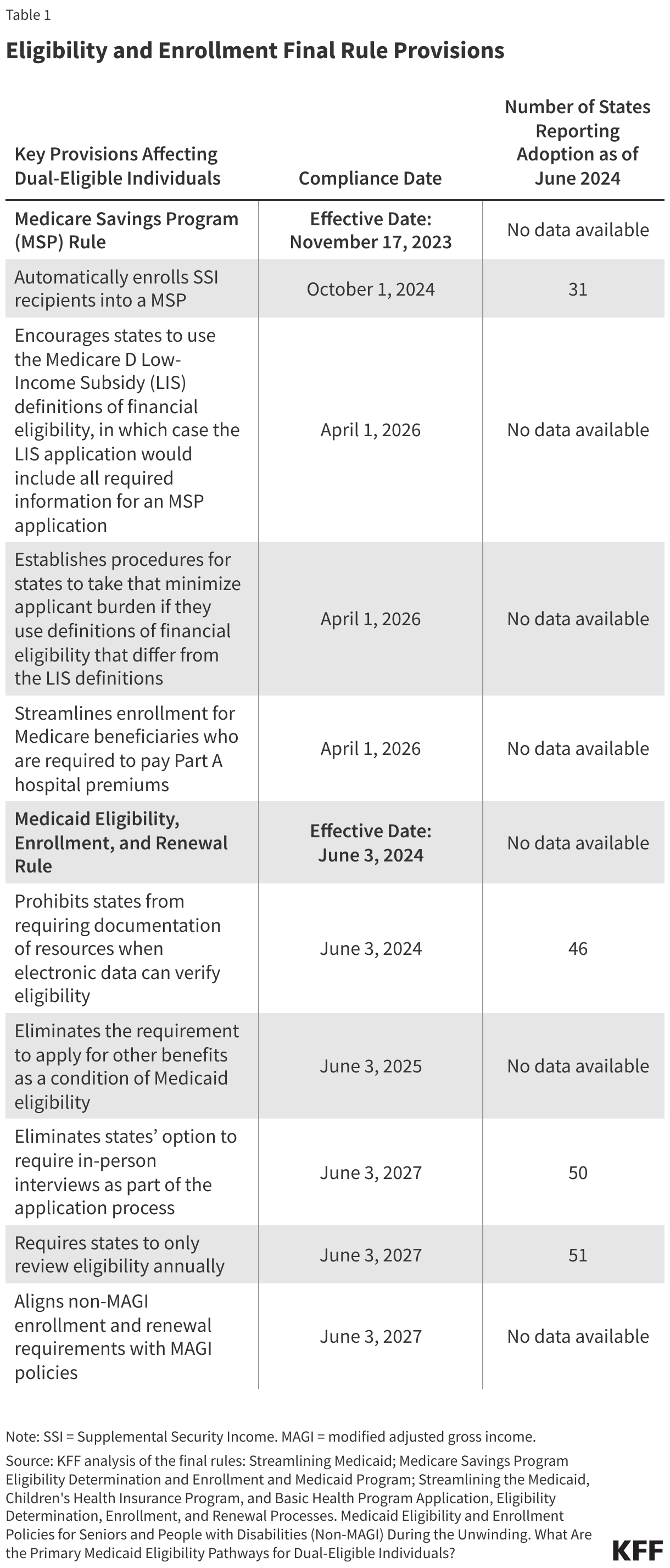
The core of the issue lies in the delay—or permanent erasure—of two federal rules designed to streamline the enrollment process. By minimizing the "administrative burden"—the paperwork, in-person interviews, and verification hurdles—these rules were intended to ensure that eligible individuals stayed enrolled. The proposed legislation seeks to undo these protections, effectively raising the wall between low-income patients and the coverage they are legally entitled to.
Supporting Data: The Anatomy of Enrollment Loss
The scale of the projected disenrollment is staggering. The CBO estimates that the delay of these two administrative rules alone accounts for $167 billion in federal savings over ten years, making it the second-largest cut in the entire reconciliation package.
Data from the Kaiser Family Foundation (KFF) highlights why this is particularly dangerous for "dual-eligible" individuals—those who qualify for both Medicare and Medicaid. These individuals are typically elderly or have significant disabilities and live on fixed incomes with limited savings. Research shows that even under current, more streamlined systems, 28% of newly eligible dual-enrollees lose their Medicaid coverage within the first year. By reinstating the administrative barriers that these rules sought to remove, the legislation creates a "leaky bucket" effect where coverage is lost not due to a change in financial eligibility, but due to an inability to navigate complex bureaucratic requirements.
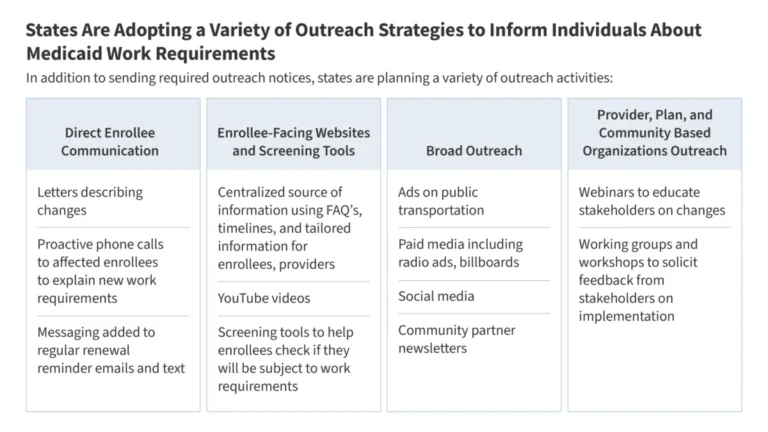
The impact is compounded by the behavior of individual states. Currently, 38 states use pre-populated renewal forms for seniors and individuals with disabilities—a "best practice" that makes it easier to verify continued eligibility. If the federal mandate for these streamlined processes is removed, many states are expected to revert to older, more cumbersome practices, such as requiring paper documentation or mandatory in-person interviews, which serve as significant deterrents to re-enrollment.
The Reality of "Dual-Eligibility" and Financial Strain
To understand the human impact, one must look at the financial arithmetic of a dual-eligible beneficiary. Medicare, while robust, is not free. It carries premiums, deductibles, and cost-sharing requirements that can be prohibitive for someone on Supplemental Security Income (SSI).
In 2025, the monthly Part B premium for Medicare is $185. For an individual receiving a monthly SSI benefit of $967, that premium represents nearly 20% of their total income. Medicaid Savings Programs (MSPs) traditionally cover these premiums and cost-sharing, acting as a critical financial bridge. When a beneficiary loses Medicaid due to administrative hurdles, they do not lose their Medicare, but they suddenly become responsible for costs they cannot afford.
The loss of this coverage extends to essential benefits not covered by Medicare, such as long-term care, dental services, and non-emergency medical transportation. Furthermore, there is the issue of the Medicare Part D Low-Income Subsidy (LIS). When individuals are disenrolled from Medicaid, they are often inadvertently cut off from the LIS, leading to a "double hit" where they must suddenly pay for both their medical premiums and their prescription drug costs. This is not a theoretical risk; between December 2024 and January 2025, the number of LIS recipients dropped by 1 million, directly following the "unwinding" of the Medicaid continuous enrollment provision.
Official Responses and Political Implications
The debate has sparked a firestorm in Washington. Proponents of the legislation, largely within the House majority, argue that these administrative rules constitute federal overreach and that states should have the flexibility to determine their own enrollment verification processes to prevent "waste, fraud, and abuse." They contend that the savings generated by these measures are essential to balancing the budget and extending tax cuts that stimulate the broader economy.
Conversely, health policy experts and advocacy groups argue that these "administrative burdens" are a form of soft-denial of care. In a letter to leadership, critics noted that the CBO itself anticipates $11 billion in reduced Medicare spending—not because the beneficiaries have improved health, but because the increased cost-sharing will force them to forgo care altogether.
The Senate’s move to prohibit the rules entirely has drawn the ire of healthcare providers who argue that the legislative focus is misplaced. By focusing on administrative costs, lawmakers are effectively targeting the most vulnerable, who lack the resources to hire advocates to help them navigate the re-enrollment process.
Long-term Implications for the Healthcare Ecosystem
The ripple effects of this legislation will likely be felt far beyond the balance sheets of the federal government. For hospitals and nursing facilities, a surge in "uncompensated care" is a distinct possibility. When patients lose their Medicaid coverage, they become "self-pay" patients in name only; their actual ability to pay remains near zero, leading to an increase in bad debt for healthcare providers who treat dual-eligible populations.
Furthermore, the public health implications are significant. When low-income seniors and the disabled stop seeing their doctors because they can no longer afford the co-pays or the transportation to get there, their conditions—often chronic—tend to deteriorate. This leads to more frequent emergency room visits and hospitalizations, which are significantly more expensive than the preventative care that Medicaid currently funds.
As the reconciliation bill moves closer to a potential final vote, the choice before Congress is clear: prioritize a specific fiscal target at the expense of millions of the most vulnerable, or preserve the administrative guardrails that ensure low-income Americans can access the healthcare they have been promised.
The data is clear. The administrative barriers proposed in the "One Big Beautiful Bill Act" are not merely procedural adjustments; they are a systemic dismantling of access for those who need it most. As the nation watches, the outcome of this legislation will serve as a definitive statement on the federal government’s commitment to its most vulnerable citizens in the coming decade.