In the complex landscape of otolaryngology, few conditions present as persistent a diagnostic challenge as the seromucinous hamartoma (SH). A benign, tumor-like malformation, SH remains an enigmatic entity for many clinicians and pathologists alike. Despite its formal recognition in the World Health Organization’s (WHO) Classification of Head and Neck Tumours, the lesion’s rarity and the frequency of "nondiagnostic" biopsy results have created a clinical blind spot.
A recent case report highlights the critical intersection of surgical strategy, diagnostic pathology, and the necessity of clinical awareness in managing these elusive nasal masses. By examining the journey of a 52-year-old patient, medical experts are shedding new light on why SH remains frequently underdiagnosed and how the medical community can refine its approach to ensure patient safety and avoid unnecessary diagnostic delays.
1. The Anatomy of a Diagnostic Dilemma: Main Facts
Hamartomas are defined by a disorganized proliferation of mature tissue elements that are native to the site of origin. Unlike true neoplasms, they lack destructive infiltrative growth. Within the sinonasal tract, hamartomatous lesions include Respiratory Epithelial Adenomatoid Hamartoma (REAH), Chondro-osseous Respiratory Epithelial Adenomatoid Hamartoma (COREAH), and the rarest of them all: Seromucinous Hamartoma (SH).
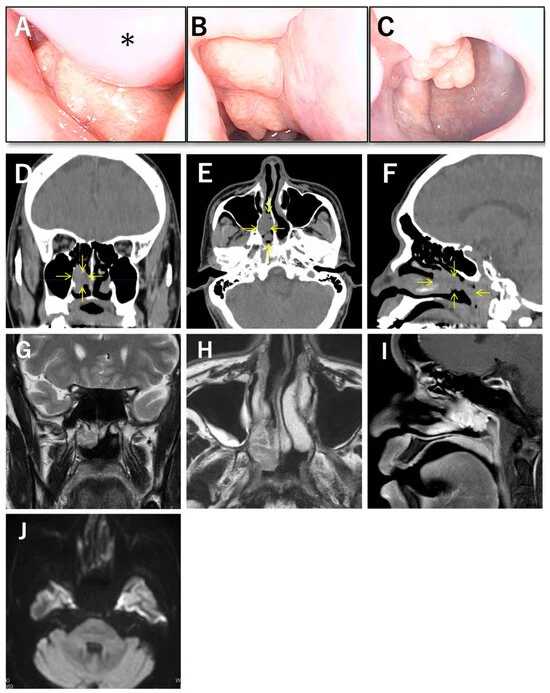
The primary challenge with SH is its presentation. Most patients report nonspecific symptoms—nasal obstruction, rhinorrhea, or postnasal discomfort—that mimic common inflammatory conditions like chronic rhinosinusitis or benign polyps. Imaging, including CT and MRI, often shows a well-circumscribed, soft-tissue lesion, but these findings lack the "pathognomonic" specificity that would allow a radiologist or surgeon to definitively identify the mass before surgery.

The crux of the clinical dilemma lies in the biopsy. Because the lesion is typically covered by a layer of intact, non-atypical respiratory epithelium, a superficial biopsy often retrieves only inflammatory cells or edematous tissue, failing to reach the deeper, diagnostic glandular structures.
2. Chronology of a Case: From Incidental Finding to Surgical Resolution
The case recently detailed by researchers serves as a textbook example of the diagnostic hurdles associated with SH.
- Initial Discovery: A 52-year-old man was found to have a mass in the posterior right nasal cavity during a routine upper gastrointestinal endoscopy performed via the nasal route. At the time, the patient was asymptomatic, and the lesion was left untreated.
- The Diagnostic Gap: Over the following year, the patient developed persistent nasal obstruction. He sought care at a community hospital, where imaging and a biopsy were performed. The imaging suggested a benign process, but the biopsy returned as nondiagnostic, failing to identify any specific glandular proliferation.
- Referral and Evaluation: The patient was referred to a specialized center. Laboratory investigations, including IgG4 levels and squamous cell carcinoma antigen tests, were within normal limits, effectively ruling out systemic inflammatory diseases or epithelial malignancies.
- Surgical Intervention: Given the persistence of symptoms and the uncertainty of the diagnosis, the surgical team opted for an endoscopic endonasal approach. To ensure a clean field, they first performed a septoplasty.
- The Procedure: Surgeons identified a 35 mm lobulated mass originating from the middle meatus. To ensure oncological safety, they performed intraoperative frozen-section analysis on the surrounding mucosa. Once malignancy was ruled out, they successfully performed an en bloc resection, carefully managing the sphenopalatine artery during the process.
- Definitive Diagnosis: Postoperative histopathological examination revealed the tell-tale irregular proliferation of mixed serous and mucinous glands—the definitive signature of SH. The patient recovered fully, with no signs of recurrence at the six-month follow-up.
3. Supporting Data and Pathological Context
The pathology of SH is fundamentally different from other sinonasal lesions. While REAH is characterized by glandular invaginations with thickened, hyalinized basement membranes, SH is defined by the proliferation of small serous and mucinous glands within the subepithelial stroma.
The data from this case underscores a vital lesson: location matters. Because the diagnostic elements of the lesion lie deep within the subepithelial tissue, the standard office-based biopsy—which is often kept shallow to avoid bleeding in the posterior nasal cavity—is structurally incapable of capturing the necessary pathology.

Furthermore, the imaging data provides a "non-aggressive" profile. The absence of bone destruction, the lack of restricted diffusion on MRI, and the relatively uniform enhancement pattern serve as clinical indicators that steer the surgeon away from aggressive resection but also prevent a definitive preoperative label.
4. Official Perspectives and Clinical Implications
The medical community, led by guidelines in the WHO Classification of Head and Neck Tumours, acknowledges that the scarcity of SH cases is partly due to underrecognition. The implications for clinicians are profound:
A. The Necessity of Clinical-Pathological Dialogue
Surgeons must provide pathologists with more than just a tissue sample. When a clinician suspects a hamartomatous lesion based on a smooth, lobulated, posterior nasal mass, this context is vital. Pathologists who are aware of the clinical appearance of the lesion are better equipped to look for the specific glandular proliferation that might otherwise be dismissed as nonspecific inflammation.
B. Rethinking Biopsy Techniques
The current standard for office-based biopsies may need to be revisited for suspected SH. When a lesion is located in the posterior nasal cavity and remains unclassified after an initial attempt, practitioners should consider:

- Using more substantial sampling instruments.
- Targeting the base of the lesion rather than the superficial surface.
- Moving toward surgical excision under general anesthesia as a diagnostic-therapeutic hybrid, especially when the patient remains symptomatic.
C. Surgical Strategy
Endoscopic surgery has become the preferred route for SH. However, as this case demonstrates, it is not merely a matter of "removing a polyp." Surgeons must account for vascular structures, such as the sphenopalatine artery, and utilize intraoperative frozen sections to define the resection margins. The goal is en bloc removal to ensure that the architecture of the lesion is preserved for final analysis, which also aids in ruling out rare instances of malignant transformation.
5. Conclusion: A Call for Greater Awareness
The case of the 52-year-old patient is more than a successful surgery; it is a clinical call to action. The persistence of SH as a diagnostic dilemma is driven by a cycle of caution—where clinicians, afraid of complications in the deep nasal cavity, take small biopsies that the pathologist, in turn, cannot diagnose.
By recognizing that SH should be part of the differential diagnosis for any non-aggressive, lobulated posterior nasal mass, the medical community can move toward a more proactive management style. When biopsies are nondiagnostic, surgeons should not assume the lesion is merely an inflammatory polyp. Instead, they should treat the diagnostic ambiguity as a clinical finding in itself, warranting a more thorough investigation or definitive surgical removal.
As more cases are accurately documented and the pathology is better understood, the medical field will continue to demystify this rare entity, ultimately improving patient outcomes and streamlining the path from symptom to definitive diagnosis.