A groundbreaking study published in the journal Cancers offers a beacon of hope for patients undergoing complex megaprosthetic reconstructions, particularly those at risk of periprosthetic joint infection (PJI). Researchers have demonstrated that synovial calprotectin, a readily available biomarker measured in joint fluid, exhibits high diagnostic accuracy in identifying these challenging infections, even in the presence of confounding factors that often render traditional diagnostic methods unreliable.
The findings from a tertiary sarcoma center indicate that synovial calprotectin could become an invaluable tool for orthopedic oncologists and surgeons, aiding in the swift and accurate diagnosis of PJI following tumor resection and megaprosthetic reconstruction. This development is crucial, as accurately diagnosing and managing PJI in these intricate cases is notoriously difficult, often leading to delayed treatment, unnecessary surgeries, and poorer patient outcomes.
The Challenge of Diagnosing Periprosthetic Joint Infection in Megaprostheses
Megaprosthetic reconstructions, vital for limb salvage after bone tumor removal, are inherently complex and carry a significant risk of complications, with periprosthetic joint infection (PJI) being a major concern. Infection rates in these cases can exceed 20%, a figure considerably higher than in standard joint replacements. The intricate nature of these reconstructions, often involving extensive soft-tissue compromise and prior oncological treatments, complicates the host’s inflammatory response, rendering conventional diagnostic markers like blood tests and standard joint fluid analysis less effective.

This diagnostic ambiguity frequently leads to inconclusive results when using established criteria, such as the 2018 International Consensus Meeting (ICM) guidelines, which were primarily developed for routine arthroplasty. Such uncertainty can result in delayed treatment for true infections or, conversely, lead to high-risk revision surgeries for aseptic complications. The need for a reliable, rapid, and accessible diagnostic tool in this specific patient population has been paramount.
Synovial Calprotectin: A New Frontier in Diagnostic Accuracy
The study, led by Vasileios Kontogeorgakos and his team, prospectively evaluated 20 consecutive patients with tumor-related megaprosthetic reconstructions who presented with suspected PJI. The primary focus was on assessing the diagnostic performance of synovial calprotectin, a protein released by neutrophils, which is known to be elevated in infected joint fluid. The researchers utilized a rapid lateral-flow assay (LFA) for calprotectin measurement, providing results within minutes.
Key findings from the study include:
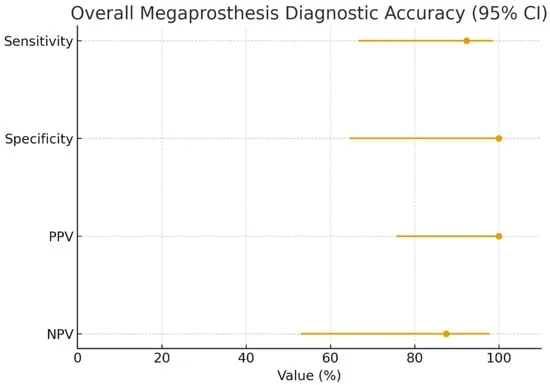
- High Sensitivity and Specificity: Synovial calprotectin, using a threshold of ≥50 mg/L, demonstrated a sensitivity of 92.3% and a specificity of 100% in identifying PJI in the megaprosthesis cohort. This indicates a strong ability to correctly identify infected cases and, crucially, to rule out infection with high confidence.
- No False Positives: The absence of false-positive results is particularly significant, as it suggests that a positive calprotectin test in this context is highly indicative of actual infection, minimizing the risk of unnecessary interventions.
- Excellent Rule-Out Capability: The negative predictive value (NPV) of 87.5% further underscores the test’s utility in excluding infection, providing reassurance to clinicians and potentially avoiding high-morbidity revision surgeries for patients without infection.
- Performance in Challenging Subgroups: The biomarker maintained its strong diagnostic performance even in patients with low C-reactive protein (CRP) levels (<10 mg/L). This is a critical finding, as low CRP can be misleading in patients with compromised immune systems or in the aftermath of prior treatments, making standard inflammatory markers less informative.
- Agreement with Existing Criteria: Synovial calprotectin showed substantial agreement (Cohen’s κ = 0.76) with the 2018 ICM infection classification. Furthermore, it successfully clarified two out of three cases that were deemed inconclusive by the ICM criteria, offering a valuable solution to diagnostic ambiguity.
- Exploratory Comparative Analysis: In an exploratory matched comparison with a cohort of non-megaprosthesis arthroplasty patients, calprotectin exhibited comparable diagnostic accuracy, suggesting its utility extends beyond the complex megaprosthesis setting.
Chronology of the Study and Findings
The research, conducted at the ATTIKON University General Hospital in Athens, Greece, involved a prospective observational design. Patients were enrolled from September 2023, with all participants undergoing diagnostic synovial fluid aspiration and subsequent revision surgery. The minimum follow-up period of one year ensured accurate determination of infection status.
The study’s timeline can be broken down as follows:
- Submission Received: March 31, 2026
- Revised: April 30, 2026
- Accepted: May 1, 2026
- Published: May 8, 2026
The rigorous methodology involved the collection of comprehensive clinical and laboratory data, with a focus on a composite reference standard for infection adjudication that included intraoperative findings and microbiological cultures. The researchers meticulously analyzed the diagnostic accuracy metrics, ensuring adherence to STARD 2015 guidelines.

Supporting Data and Microbiological Insights
The study provided detailed insights into the characteristics of the infected megaprosthesis cohort. Among the 13 infected patients, coagulase-negative staphylococci (CoNS) were the most prevalent pathogens, accounting for 61.5% of infections, with Staphylococcus epidermidis and Staphylococcus haemolyticus being the most frequently isolated species. Staphylococcus aureus was identified in 23.1% of cases, and polymicrobial infections were present in 30.8% of infected patients. This detailed microbiological profile highlights the diverse infectious agents that can compromise these complex reconstructions.
The statistical analysis, including the calculation of sensitivity, specificity, positive and negative predictive values, and likelihood ratios, provided robust evidence for calprotectin’s diagnostic power. The area under the receiver operating characteristic (ROC) curve (AUC) of 1.00 for continuous calprotectin values, while requiring cautious interpretation due to the sample size, is a strong indicator of excellent discriminatory ability.
Official Responses and Clinical Implications
While direct official responses from regulatory bodies or major orthopedic societies are not yet available, the implications of this research are significant for the field of orthopedic oncology and reconstructive surgery. The findings are expected to influence clinical guidelines and diagnostic protocols for managing suspected PJI in megaprosthesis patients.

The study’s authors, including Panayiotis Gavriil, Panagiotis Briassoulis, Jendrik Hardes, Panayiotis Papagelopoulos, and Vasileios Kontogeorgakos, emphasize that synovial calprotectin should be viewed as a valuable adjunctive biomarker. Its rapid turnaround time and ease of use with an LFA make it particularly attractive for point-of-care decision-making, especially in settings where immediate diagnostic clarity is critical.
Broader Implications and Future Directions
The successful application of synovial calprotectin in the challenging context of megaprosthetic reconstructions opens avenues for further research and clinical implementation. The study’s authors advocate for larger, multicenter validation studies to confirm these findings and to potentially refine optimal diagnostic thresholds for this specific patient population. Further investigation into the role of calprotectin in differentiating between infectious and aseptic implant loosening, particularly in the context of advanced implant wear and osteolysis, would also be beneficial.
In conclusion, this pioneering study offers a promising new diagnostic avenue for a vulnerable patient group. By providing a reliable and accessible tool for identifying periprosthetic joint infections, synovial calprotectin has the potential to significantly improve diagnostic accuracy, guide timely treatment decisions, and ultimately enhance outcomes for patients undergoing complex megaprosthetic reconstructions. The findings represent a crucial step forward in addressing the diagnostic challenges inherent in this specialized area of orthopedic surgery.