The landscape of oncology is shifting. For decades, a breast cancer diagnosis was often met with a singular, aggressive approach. Today, the medical community understands that breast cancer is not a monolithic disease but a collection of distinct subtypes, each requiring a unique roadmap for treatment. Among these, Hormone Receptor-positive (HR+) breast cancer stands as the most prevalent, accounting for approximately 70% of all cases in women.
While the sheer frequency of this diagnosis can be daunting, the narrative surrounding HR-positive breast cancer has transformed into one of profound optimism. Driven by decades of rigorous research and a recent surge in pharmacological breakthroughs, HR-positive breast cancer has become one of the most treatable and manageable forms of the disease.
Main Facts: Defining the HR-Positive Subtype
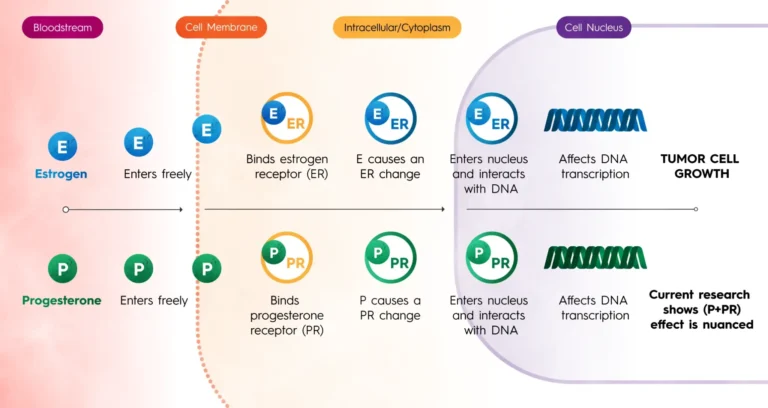
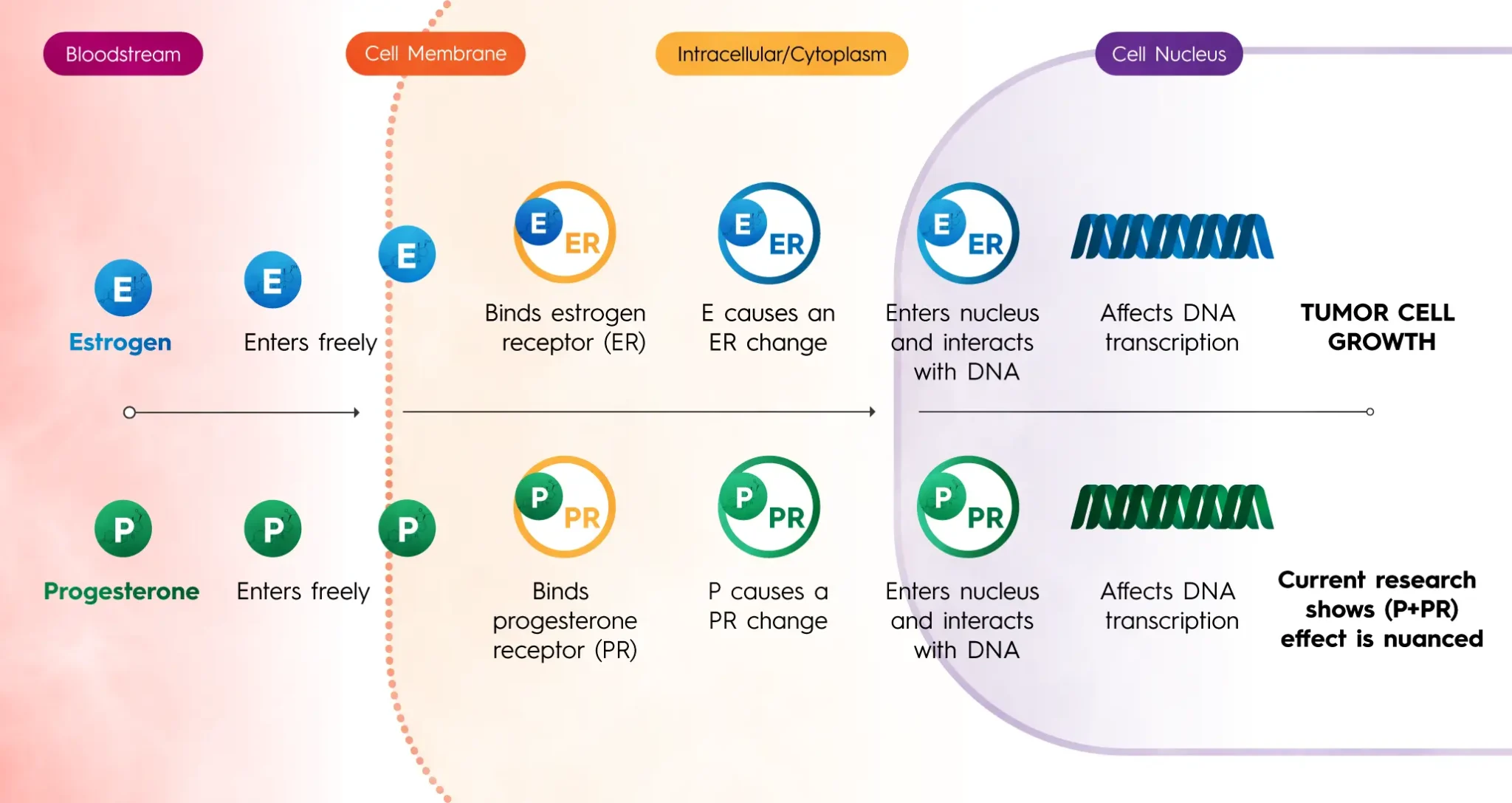
To understand why HR-positive breast cancer is unique, one must look at the cellular level. In this subtype, cancer cells possess specific proteins—receptors—that are sensitive to the hormones estrogen, progesterone, or both. These hormones, which occur naturally in the body, act as biological fuel. When they bind to the receptors on the tumor cells, they send signals that command the cells to grow, divide, and spread.
Medical professionals classify these tumors based on which receptors are present:
- ER-positive (ER+): The cells have receptors for estrogen.
- PR-positive (PR+): The cells have receptors for progesterone.
- Double Positive: Most HR-positive cancers are both ER- and PR-positive.
The presence of these receptors is the "Achilles’ heel" of the tumor. Because the cancer depends on hormonal signals to thrive, doctors can deploy endocrine therapies designed to either block these receptors or lower the body’s hormone production entirely. This targeted approach is fundamentally different from traditional chemotherapy, which attacks all rapidly dividing cells; endocrine therapy specifically starves the cancer of its primary food source.
Chronology: A Half-Century of Progress
The journey from rudimentary treatments to precision medicine in HR-positive breast cancer has followed a clear, accelerating timeline:
The 1970s: The Tamoxifen Revolution
The first major breakthrough came with the development of Tamoxifen, a Selective Estrogen Receptor Modulator (SERM). Approved in the 1970s, it changed the prognosis for millions by preventing estrogen from binding to cancer cells. It remains a gold standard for premenopausal women today.
The 1990s and 2000s: The Rise of Aromatase Inhibitors (AIs)
Researchers realized that for postmenopausal women, estrogen is produced differently—primarily through the conversion of androgens in fatty tissue rather than in the ovaries. This led to the development of Aromatase Inhibitors (AIs) like letrozole and anastrozole, which block the enzyme responsible for this conversion.
2002: The Introduction of Fulvestrant
For twenty years, Fulvestrant was the only Selective Estrogen Receptor Downregulator (SERD) available. Unlike Tamoxifen, which blocks the receptor, Fulvestrant binds to and destroys it. However, it required monthly, often painful injections, highlighting a need for more patient-friendly options.
2015–2020: The CDK4/6 Era
The discovery of Cyclin-Dependent Kinase (CDK) 4/6 inhibitors—such as palbociclib, ribociclib, and abemaciclib—marked a paradigm shift for advanced and metastatic HR-positive cancer. These drugs, when paired with endocrine therapy, significantly extended progression-free survival by halting the cell cycle.
2023–Present: The Oral SERD and ADC Breakthroughs
In 2023, elacestrant became the first oral SERD to gain FDA approval, ending a two-decade drought in the class. This was followed by imlunestrant. Simultaneously, the rise of Antibody-Drug Conjugates (ADCs) has provided a "Trojan Horse" method for delivering chemotherapy directly to cancer cells, sparing healthy tissue.
Supporting Data: Prevalence and Prognosis
Data from the Breast Cancer Research Foundation (BCRF) and the National Cancer Institute (NCI) underscore the prevalence of this subtype. HR-positive breast cancer is most commonly diagnosed in postmenopausal women, as cumulative lifetime exposure to estrogen is a primary risk factor. However, it also accounts for the majority of breast cancer cases in men.
Key statistical insights include:
- Survival Rates: When caught early (Stage I or II), the five-year survival rate for HR-positive breast cancer exceeds 90% in many clinical cohorts, largely due to its responsiveness to endocrine therapy.
- The 70% Factor: Because it is the most common subtype, the bulk of research funding and clinical trials are focused here, leading to a robust pipeline of new drugs.
- Duration of Care: Unlike other cancers where treatment may last six months, HR-positive patients are often advised to remain on endocrine therapy for 5 to 10 years. Data shows that this "extended adjuvant therapy" significantly reduces the risk of late recurrence.
- Genomic Utility: Tools like the Oncotype DX and MammaPrint assays have revolutionized decision-making. By analyzing the expression of 21 or more genes in a tumor, these tests provide a "recurrence score." Data indicates that many women with low-risk HR-positive cancer can safely skip chemotherapy entirely, avoiding its toxic side effects.
Official Responses: Insights from the Scientific Community
Organizations like the Breast Cancer Research Foundation (BCRF) emphasize that the current "cause for optimism" is the direct result of sustained, investigator-led research.
"The progress we see today in HR-positive breast cancer—specifically the transition from injectable to oral SERDs and the success of CDK4/6 inhibitors—is a testament to decades of foundational science," a spokesperson for the research community noted. "We are no longer just treating the cancer; we are outsmarting its resistance mechanisms."
Medical experts also highlight the "nuanced" safety profiles of the latest drugs. While chemotherapy often causes hair loss and severe immune suppression, the newer oral SERDs and targeted therapies are generally well-tolerated. This allows patients to maintain a high quality of life while managing their disease as a chronic condition rather than an acute crisis.
However, officials also sound a note of caution regarding "late recurrence." Because HR-positive tumors can grow slowly, they have a unique ability to remain dormant and return 10, 15, or even 20 years later. This reality is why the oncology community remains steadfast in recommending long-term follow-up and adherence to hormone therapy regimens.
Implications: The Future of Personalized Care
The evolution of HR-positive breast cancer treatment has profound implications for the future of medicine.
1. The End of "One Size Fits All"
The ability to use genomic testing to determine who needs chemotherapy and who doesn’t represents a move toward truly personalized medicine. This reduces the economic and physical burden on patients who would not benefit from aggressive "slash and burn" treatments.
2. Managing Resistance
The biggest hurdle in HR-positive care is "endocrine resistance," where the cancer eventually learns to grow despite hormone blockades. The arrival of next-generation drugs like ADCs and PI3K inhibitors (like alpelisib) means that doctors now have a "second and third line" of defense. If one treatment stops working, there are now multiple backups available.
3. Patient Empowerment and Quality of Life
The shift toward oral medications (like oral SERDs) means fewer hospital visits and less invasive procedures. For a patient who must be on treatment for a decade, the difference between a daily pill and a monthly injection is significant for their mental health and autonomy.
4. The Role of Long-Term Monitoring
The risk of late recurrence implies that the relationship between a patient and their oncology team must be a long-term partnership. It also signals a need for further research into "dormancy"—understanding how cancer cells sleep for years and what triggers them to wake up.
5. A Model for Other Cancers
the success of targeting the hormone receptor in breast cancer serves as a blueprint for other hormone-driven diseases, such as prostate cancer. The "targeted approach" pioneered here is the gold standard for modern drug development.
Conclusion
For those navigating a diagnosis of HR-positive breast cancer today, the message is clear: knowledge is the most potent tool in the arsenal. While the diagnosis is life-changing, the scientific trajectory is moving toward a future where breast cancer is either cured early or managed effectively for a lifetime.
Through the continued efforts of organizations like the BCRF and the participation of thousands of women in clinical trials, the "fuel" that once drove tumor growth is being systematically cut off. The toolkit is larger, the drugs are smarter, and the outlook has never been brighter. In the fight against HR-positive breast cancer, science is not just keeping pace—it is winning.