Editorial Note
Originally established in November 2009, this comprehensive analysis is updated periodically to reflect the shifting landscape of global health policy, evolving legislative frameworks, and the current administrative posture regarding the U.S. commitment to combating HIV/AIDS.
Executive Summary: The Global HIV Landscape
HIV/AIDS remains one of the most formidable challenges to global public health and socioeconomic development in the modern era. Despite decades of scientific and diplomatic progress, the crisis persists with approximately 40.8 million people currently living with HIV worldwide. Since the onset of the epidemic, tens of millions have succumbed to AIDS-related illnesses. While the global community has made significant strides in curbing transmission rates and increasing access to life-saving antiretroviral therapy (ART), the progress is currently at a fragile juncture.
A Chronology of Commitment and Contention
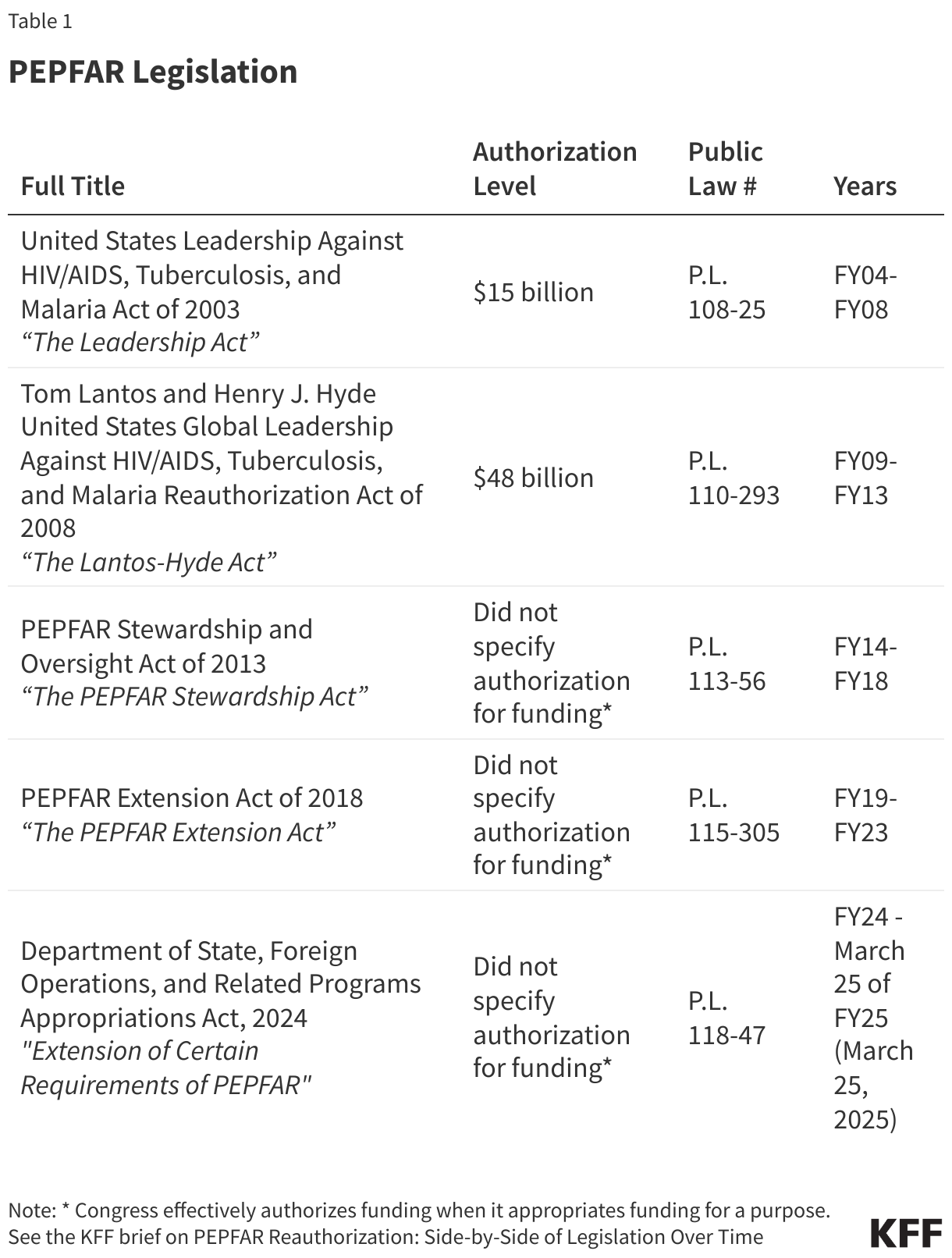
The U.S. government’s involvement in the global fight against HIV dates back to the mid-1980s, but the landscape was irrevocably altered in 2003 with the birth of the President’s Emergency Plan for AIDS Relief (PEPFAR). Announced by President George W. Bush during his State of the Union address, PEPFAR was authorized by Congress via the Leadership Act, signaling a paradigm shift in how the U.S. approached global health security.
- 2003: PEPFAR is established, becoming the largest global health program in history dedicated to a single disease.
- 2008: The Lantos-Hyde Act extends and expands the program’s scope.
- 2013 & 2018: Subsequent reauthorizations affirm bipartisan consensus on the necessity of the program.
- 2024: A period of instability begins. A short-term reauthorization in early 2024, which expired in March 2025, marked the first time the program faced significant legislative turbulence, as it became entangled in domestic political debates, particularly surrounding abortion policies.
Supporting Data: The Magnitude of the Mission
PEPFAR is credited with saving over 26 million lives since its inception. In Fiscal Year 2024, the program reached critical benchmarks:
- Testing: Supported testing services for 83.8 million individuals.
- Prevention: Prevented 7.8 million mother-to-child HIV transmissions.
- Care: Provided essential support for 6.6 million orphans and vulnerable children.
- Treatment: Sustained antiretroviral therapy for 20.6 million people.
However, the most recent fiscal data (FY 2025, Quarter 4) paints a concerning picture. While the total number of people on ART remains stable, there has been a marked decline in new enrollments, HIV testing, and the provision of Pre-Exposure Prophylaxis (PrEP). These metrics suggest that the operational momentum built over two decades is beginning to wane.
Structural Evolution and Administrative Shifts
The organizational architecture of PEPFAR was designed for efficiency and centralization. Under the Leadership Act, the Office of the Global AIDS Coordinator (OGAC) at the Department of State was tasked with oversight. The Global AIDS Coordinator, holding the rank of Ambassador, historically served as the singular voice for U.S. HIV diplomacy.
In recent years, the administrative structure has undergone a metamorphosis. Following the integration of various global health functions into the Bureau of Global Health Security and Diplomacy (GHSD), the role of specialized agencies like USAID and the CDC has been marginalized. The current strategy favors a transition toward bilateral global health agreements—broad frameworks that demand greater co-investment from host nations and signal a long-term reduction in U.S. direct financial assistance.
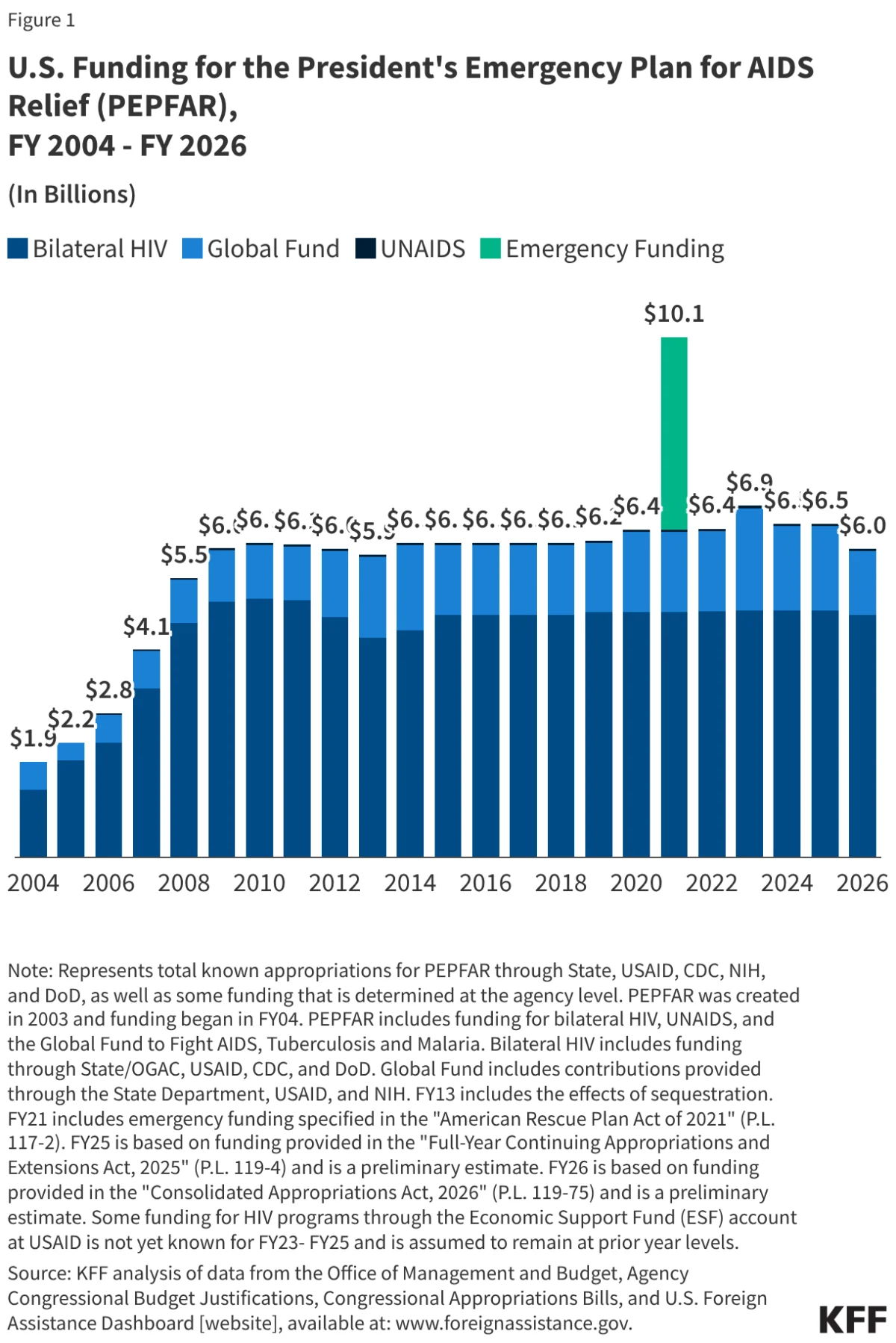
Financial Trajectory: The Price of Progress
With a cumulative appropriation exceeding $130 billion, PEPFAR represents the largest single-disease financial commitment in human history. In FY 2026, funding reached $6 billion. This expenditure has historically comprised 53-55% of the total U.S. global health budget.
Spending Directives and Congressional Oversight
Over its history, Congress has utilized "earmarks" to ensure funds were allocated toward specific high-impact areas, such as:
- Treatment and Care: Ensuring the majority of funds reach those currently living with the virus.
- Prevention: Mandating specific investments in sexual health education and commodity distribution.
- Sustainability: Encouraging the transition of service delivery to local country systems.
PEPFAR and the Global Fund: A Multilateral Synergy
Beyond its bilateral programs, the U.S. is the primary donor to the Global Fund to Fight AIDS, Tuberculosis and Malaria. Since 2001, the U.S. has contributed nearly $33 billion to the fund. This partnership is vital; while PEPFAR focuses heavily on bilateral health diplomacy, the Global Fund provides a mechanism to reach a broader array of nations and address systemic issues, including health system strengthening (HSS). The U.S. statutory limit—which restricts contributions to no more than 33% of the Global Fund’s total budget—remains a cornerstone of U.S. multilateral policy.
Official Responses and Political Implications
The shift in the political climate has fundamentally altered the trajectory of PEPFAR. The second Trump administration’s "America First" foreign aid review and the implementation of new bilateral agreements have introduced significant uncertainty.
The abandonment of the previous, consistent reauthorization model in favor of short-term, stop-gap measures has left international partners and domestic stakeholders in a state of apprehension. The politicization of the program—linking the fight against a global epidemic to domestic cultural debates—threatens to dismantle the bipartisan consensus that kept the program alive for over two decades.
Implications for the Future
The current state of PEPFAR can be described as a "controlled transition." As the U.S. pivots toward requiring partner countries to take on more fiscal responsibility, the primary concern among public health experts is the "implementation gap." Many nations currently supported by PEPFAR lack the domestic infrastructure to absorb the costs of massive HIV care programs.
The transition from the established Country Operational Plans (COPs)—which allowed for granular, data-driven management—to broad bilateral agreements may lead to a loss of oversight. If the U.S. continues to reduce its footprint without ensuring that host countries have the necessary capacity, there is a substantial risk of reversing the progress made in the last 20 years.
Furthermore, the lack of a Senate-confirmed Global AIDS Coordinator at this critical juncture leaves a vacuum in leadership. Without a clear advocate at the helm, the program’s ability to navigate diplomatic challenges and maintain the trust of international stakeholders remains severely compromised.
Conclusion: A Legacy at Risk
PEPFAR stands as a testament to the power of American leadership in global health. It has demonstrated that with sufficient political will and financial backing, humanity can turn the tide against even the most intractable diseases. However, as the program enters its third decade, the combination of legislative instability, administrative restructuring, and a shifting ideological approach to foreign aid suggests that the era of PEPFAR as the world’s gold standard in health diplomacy is undergoing a profound and potentially destabilizing transformation. The international community watches closely to see whether this "new course" will maintain the life-saving impact of the past or allow the epidemic to regain its foothold in the world’s most vulnerable populations.