
In the rapidly evolving landscape of metabolic medicine, Eli Lilly’s experimental drug, retatrutide, has emerged as a potential paradigm-shifter. As a triple hormone receptor agonist, the drug is pushing the boundaries of what is pharmacologically possible in weight management. However, as Phase 3 clinical data matures, the medical community is grappling with a dual narrative: unprecedented weight loss efficacy countered by a nuanced and occasionally challenging side-effect profile.
The Core Data: A New Benchmark for Weight Reduction
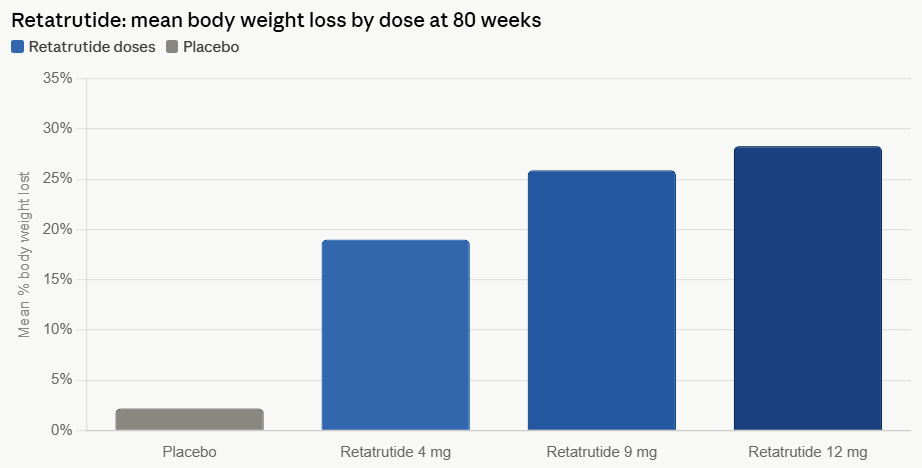
The TRIUMPH-1 Phase 3 clinical trial has delivered data that has captivated the pharmaceutical industry. At its highest tested dose (12 mg), retatrutide demonstrated an average weight loss of 28.3% over an 80-week period. This figure positions retatrutide as one of the most potent weight-loss agents currently in development, exceeding the benchmarks set by existing GLP-1 receptor agonists.
Kenneth Custer, executive vice president and president of Lilly Cardiometabolic Health, has framed the drug as a milestone in the "obesity journey." According to Custer, the flexibility of the dosing regimen—ranging from a 4 mg dose that induces significant initial weight loss to a 12 mg dose capable of mimicking the physiological outcomes of bariatric surgery—offers a "patient-centric approach."
Despite the enthusiasm surrounding its efficacy, the clinical reality is accompanied by a higher burden of adverse events. Discontinuation rates among participants receiving the highest dose reached 11.3%, a figure that surpasses the dropout rates observed in pivotal trials for tirzepatide (6.1%), semaglutide (8.0%), and orforglipron (10.3%). This data suggests that while the drug is highly effective, its tolerability may serve as a limiting factor for broad clinical adoption.
A Chronology of the Triple-Agonist Development
The development of retatrutide represents the latest iteration in a multi-year sprint to refine metabolic therapeutics.
- Early Development: Lilly’s initial focus on GLP-1 receptor agonists evolved into the exploration of dual and triple agonists. The goal was to target not just the GLP-1 receptor, but also the GIP (glucose-dependent insulinotropic polypeptide) and glucagon receptors to create a synergistic metabolic effect.
- The Phase 2 Proof-of-Concept: Early studies hinted at the drug’s potency, showing that by activating all three receptors, the body could potentially increase energy expenditure while simultaneously curbing appetite and improving metabolic signaling.
- The TRIUMPH-1 Milestone: The initiation of the Phase 3 trial was designed to confirm these findings in a larger, more diverse patient population. The 80-week data, released recently, confirmed the drug’s potential to reach the "30% weight loss threshold," a milestone previously reserved for surgical intervention.
- Competitive Landscape: Parallel to retatrutide’s progress, competitors like Novo Nordisk have been pushing forward with CagriSema. While CagriSema showed a respectable 22.7% weight loss in trials, it failed to demonstrate non-inferiority to Lilly’s own tirzepatide, leaving an opening for a more potent "triple-G" successor.
The Side Effect Profile: Navigating Dysesthesia and Muscle Loss
One of the more unexpected findings from the recent clinical data is the incidence of "dysesthesia"—an umbrella term for abnormal skin sensations such as burning, tingling, or the feeling of "pins and needles."
Approximately 12.5% of participants on the 12 mg dose reported these sensations. While researchers note that these events were largely mild to moderate and resolved over time, the frequency is markedly higher than in trials for other weight-loss medications. Orforglipron, for instance, reported this symptom in only 1.2% of participants.
The precise etiology remains a subject of intense scientific debate. One prevailing hypothesis is that the activation of glucagon or GLP-1 receptors—which are present on both central and peripheral nerves—may trigger these sensory disturbances. Another theory points to the rapid metabolic shift; the drastic reduction in caloric intake and body weight may lead to transient electrolyte imbalances or deficiencies in B-complex vitamins, both of which are critical for nerve conduction and health.
The Challenge of Lean Mass Preservation
Beyond neurological sensations, a critical area of concern for clinicians is the loss of lean tissue. Data indicates that GLP-1-based weight loss is rarely "pure" fat loss; typically, 20% to 35% of the total weight shed is muscle mass.
For a patient losing 70.3 lbs (the average on the high-dose retatrutide arm), this could equate to a loss of 14 to 24.6 lbs of lean muscle. This has sparked a "second wave" of innovation in the industry, where companies like SciWind Bio are working on injectable peptides specifically designed to promote weight loss while simultaneously preserving skeletal muscle—a development that could eventually render current protocols obsolete.
Implications for Bone Density and Metabolic Health
The connection between rapid weight loss and skeletal integrity is becoming a focal point of endocrinology research. According to a 2025 review in Nature Bone Research, rapid weight loss is associated with a 1% to 3% decline in bone mineral density (BMD) for every 10% of body weight lost.
This presents a clinical paradox: while weight loss reduces the mechanical stress on joints, it also reduces the dynamic strain on bones, which in turn signals the body to increase bone resorption. Evidence presented at the 2026 American Academy of Orthopaedic Surgeons (AAOS) meeting highlighted this risk, showing that GLP-1 users faced a 4.1% risk of osteoporosis compared to 3.2% in matched controls.
However, the "Triple-G" nature of retatrutide—specifically the activation of the GIP receptor—may offer a silver lining. Research suggests that GIP receptors are expressed on both osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells). Mechanistic reviews in The Journal of Clinical Endocrinology and Metabolism have suggested that drugs like tirzepatide, which share this GIP-activating mechanism, may exhibit a protective effect on bone health that is not seen in pure GLP-1 agonists. If this holds true for retatrutide, it could offer a significant clinical advantage in long-term safety.
Expert Consensus and Future Outlook
Industry analysts remain divided on the drug’s ultimate market position. While RBC Capital Markets’ Trung Huynh has labeled the drug’s efficacy as a "clean win" for Lilly, citing its best-in-class potential, others are more cautious.
Analysts at William Blair have suggested that the tolerability profile may confine retatrutide to a specific subset of patients—those at the higher end of the BMI spectrum who require maximum efficacy and can tolerate the increased side effects. For the general population, they argue, tirzepatide will likely remain the "gold standard" due to its superior balance of weight-loss power and gastrointestinal comfort.
As Eli Lilly prepares to release the full body composition data later this year, the medical community will be watching closely. The key will be to determine whether the benefits of extreme weight loss can be decoupled from the risks of muscle atrophy and bone density loss.
Ultimately, retatrutide represents the next chapter in a journey that is transforming obesity from a lifestyle management issue into a precision medicine field. Whether it becomes the standard-bearer for all patients or a specialized tool for the most severe cases will depend on the upcoming long-term safety data and the potential emergence of combinatorial therapies that can preserve lean mass while the drug does its metabolic work.






