The landscape of American public health coverage is undergoing its most significant transformation since the inception of the Affordable Care Act (ACA). Following a period of unprecedented enrollment growth fueled by pandemic-era protections, the Medicaid and Children’s Health Insurance Program (CHIP) programs are currently recalibrating under the weight of new federal policy mandates and the conclusion of the "unwinding" process. With national enrollment sitting at 80 million as of late 2025, policy experts, state administrators, and advocates are closely monitoring the impact of the 2025 Reconciliation Law, which introduces the most restrictive requirements in the program’s history.
Main Facts: The Current State of Enrollment
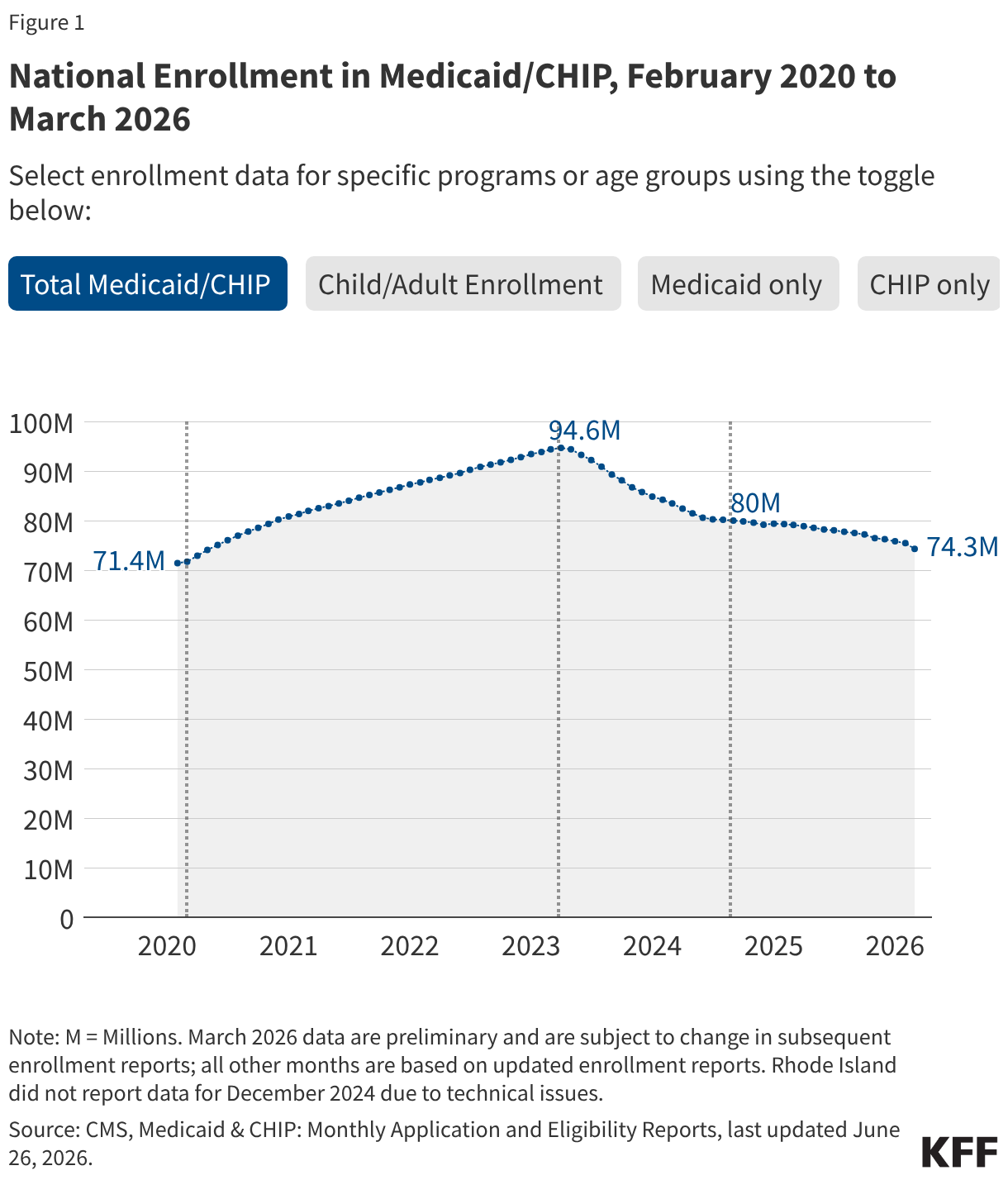
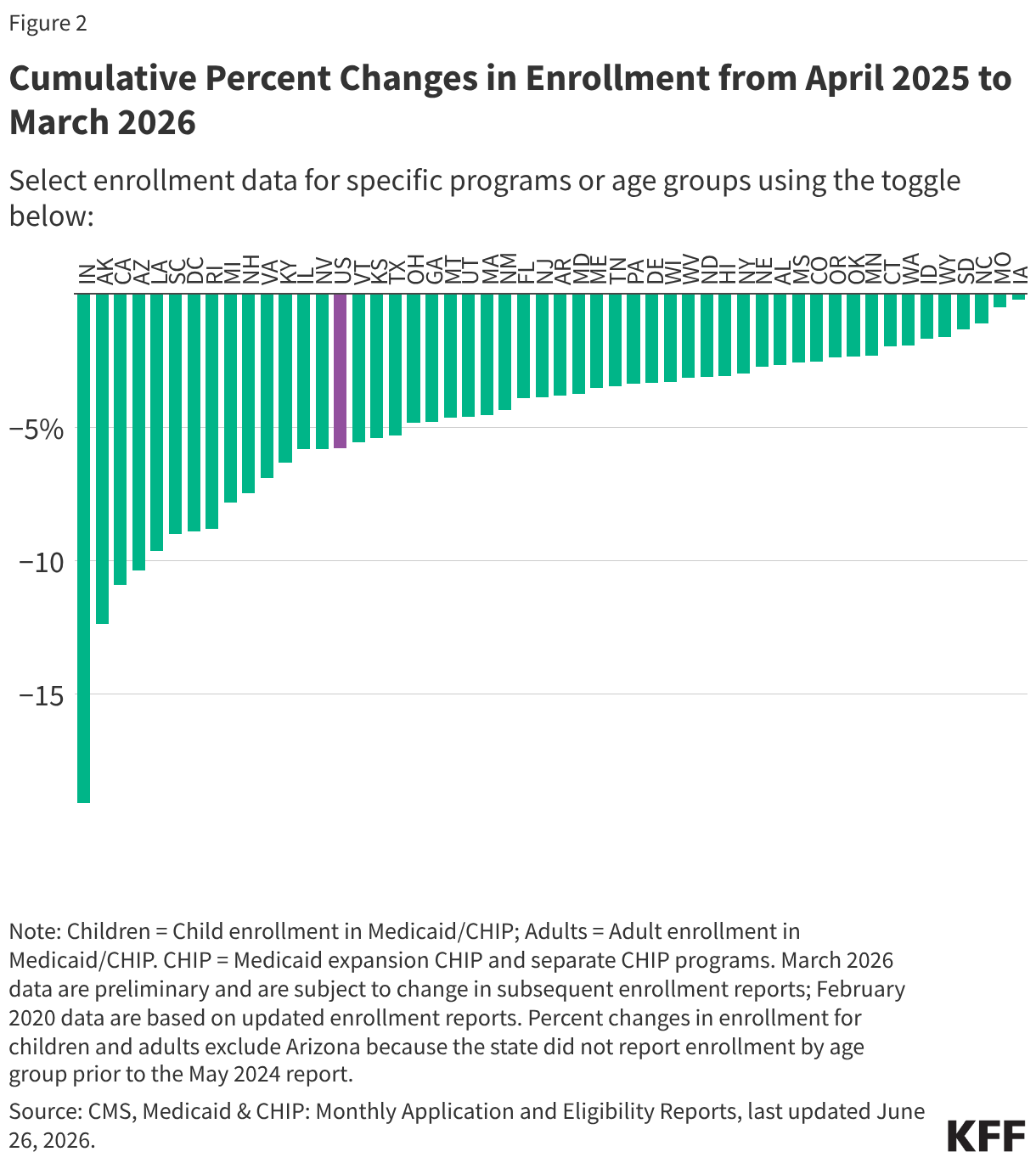
As of March 2026, the national Medicaid and CHIP enrollment landscape remains in a state of flux. While enrollment stabilized briefly in late 2024, the downward trend resumed in early 2025. Data provided by the Centers for Medicare & Medicaid Services (CMS) indicate that the post-pandemic peak of 94 million enrollees—reached in March 2023—has been significantly reduced.
It is crucial to note that current reporting metrics capture only full-benefit enrollees. This methodology excludes individuals receiving limited benefits, such as those strictly enrolled for family planning services. Consequently, these figures should be viewed as a reliable indicator of broader trends rather than a comprehensive census of every individual interacting with the Medicaid system. As the program transitions into the next phase of the 2025 Reconciliation Law, the ability to monitor specific eligibility pathways—particularly for the Medicaid expansion group—remains a critical point of concern for health equity advocates.
Chronology: From Expansion to Retrenchment
The evolution of Medicaid over the past twelve years can be categorized into four distinct phases:
The ACA Expansion Era (2014–2019)
The implementation of the Affordable Care Act’s Medicaid expansion in January 2014 fundamentally altered the program’s scope. By allowing states to cover adults with incomes up to 138% of the Federal Poverty Level (FPL), the program saw a massive influx of new enrollees. Enrollment hit a milestone of 75 million by March 2017. Following this, the program experienced a steady decline as the economy strengthened and policy priorities shifted, bottoming out at 71 million by February 2020.
The Pandemic and Continuous Enrollment (2020–2023)
The COVID-19 pandemic prompted a legislative emergency response. Congress enacted a "continuous enrollment" provision, which prohibited states from disenrolling individuals from Medicaid in exchange for enhanced federal matching funds. This act of fiscal stabilization saw enrollment surge to an all-time high of 94 million by March 2023.
The "Unwinding" Period (2023–2024)
Starting April 1, 2023, the continuous enrollment provision expired. Over the next 16 months, states embarked on the massive administrative task of redetermining eligibility for millions of enrollees. By September 2024, the national rolls had shrunk to 80 million, as states processed renewals and removed individuals deemed ineligible or those who failed to navigate the complex procedural requirements.
The 2025 Reconciliation Law and Future Hurdles (2025–Present)
The passage of the 2025 reconciliation bill has introduced a new paradigm of retrenchment. The law mandates significant policy shifts, including new work and reporting requirements for expansion enrollees, set to trigger in January 2027 (though states may opt to implement them sooner). Additionally, new restrictions on immigrant eligibility for specific coverage tiers, beginning in October 2026, are expected to exert further downward pressure on enrollment figures.

Supporting Data: Renewal Outcomes and Procedural Barriers
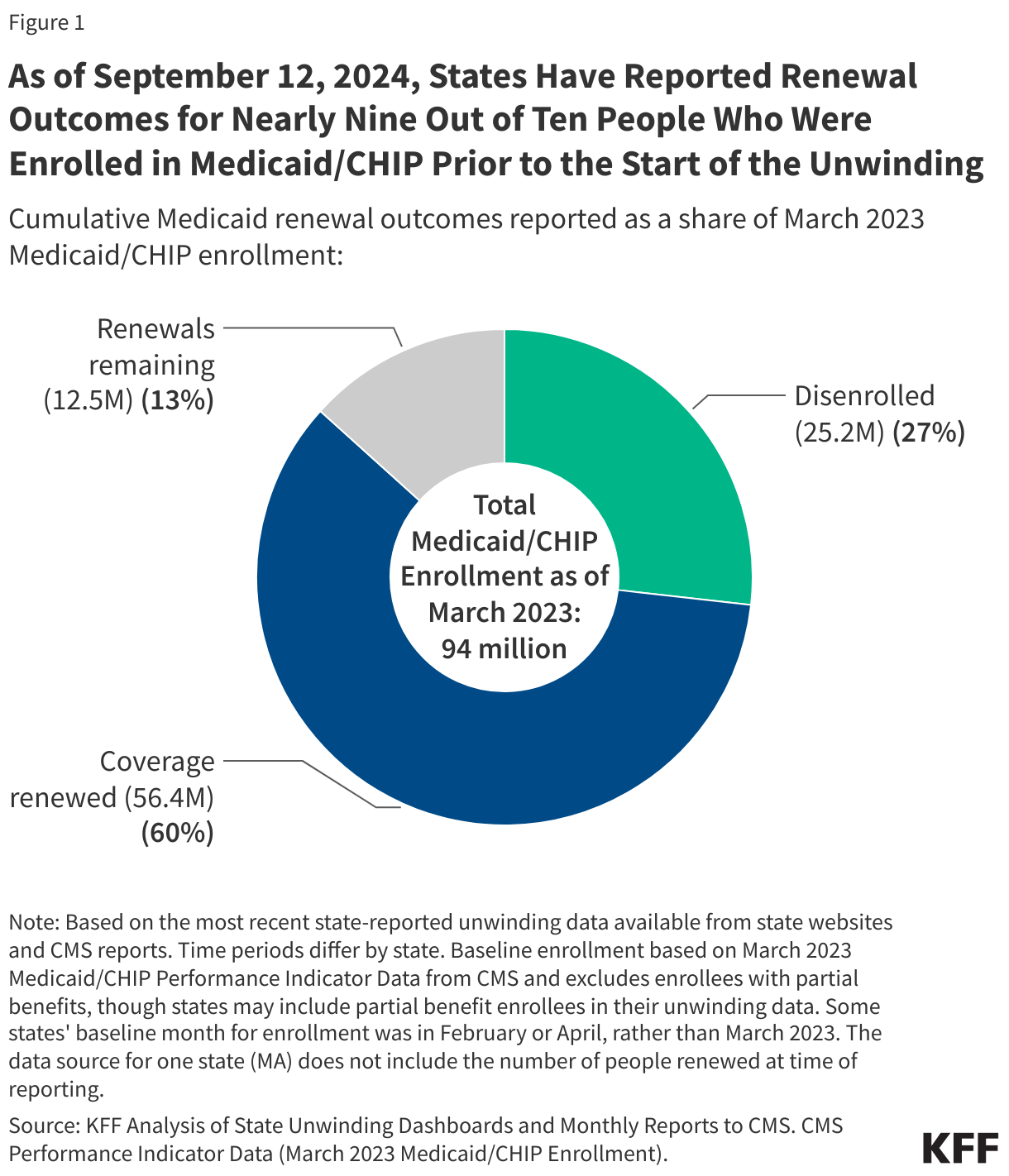
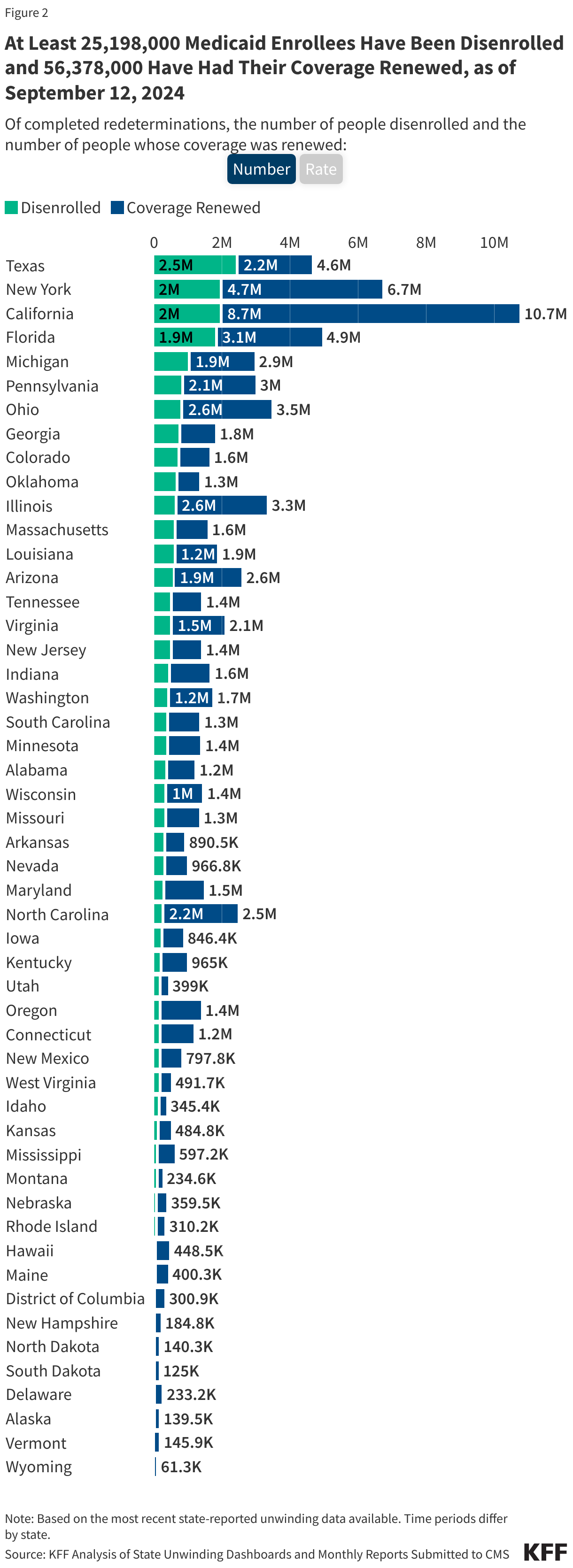
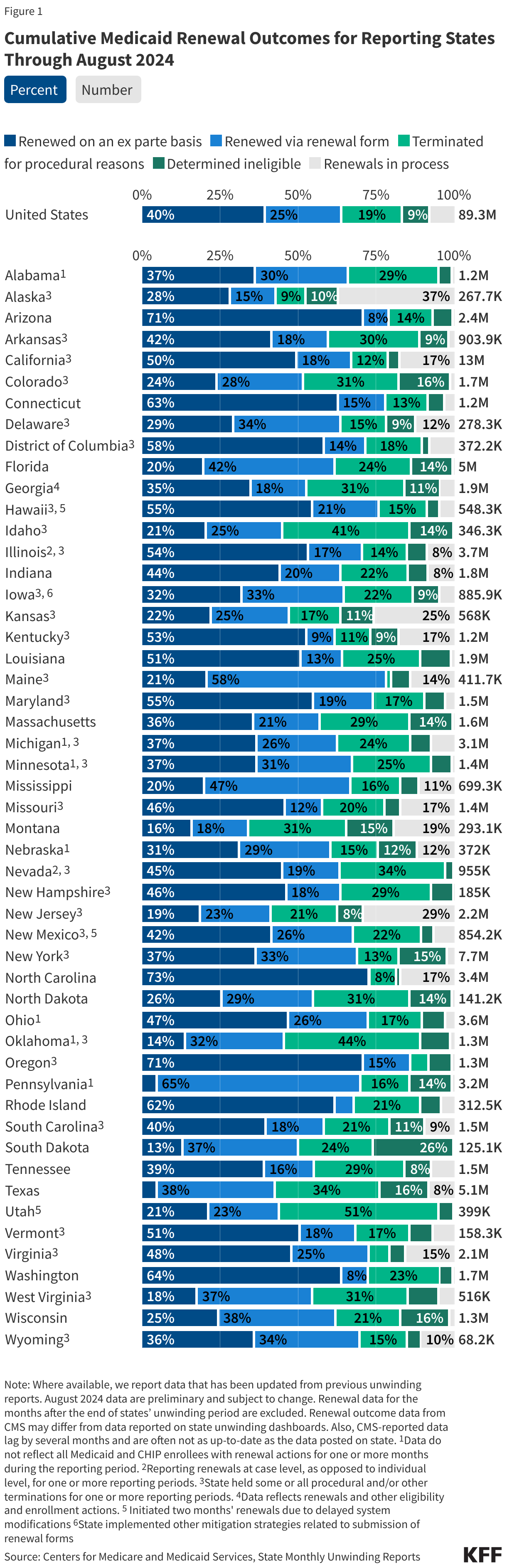
The "unwinding" of the continuous enrollment provision provided a stark look at the administrative hurdles inherent in the Medicaid system. As of September 12, 2024, nearly nine out of ten people who were enrolled prior to the unwinding had their status adjudicated.
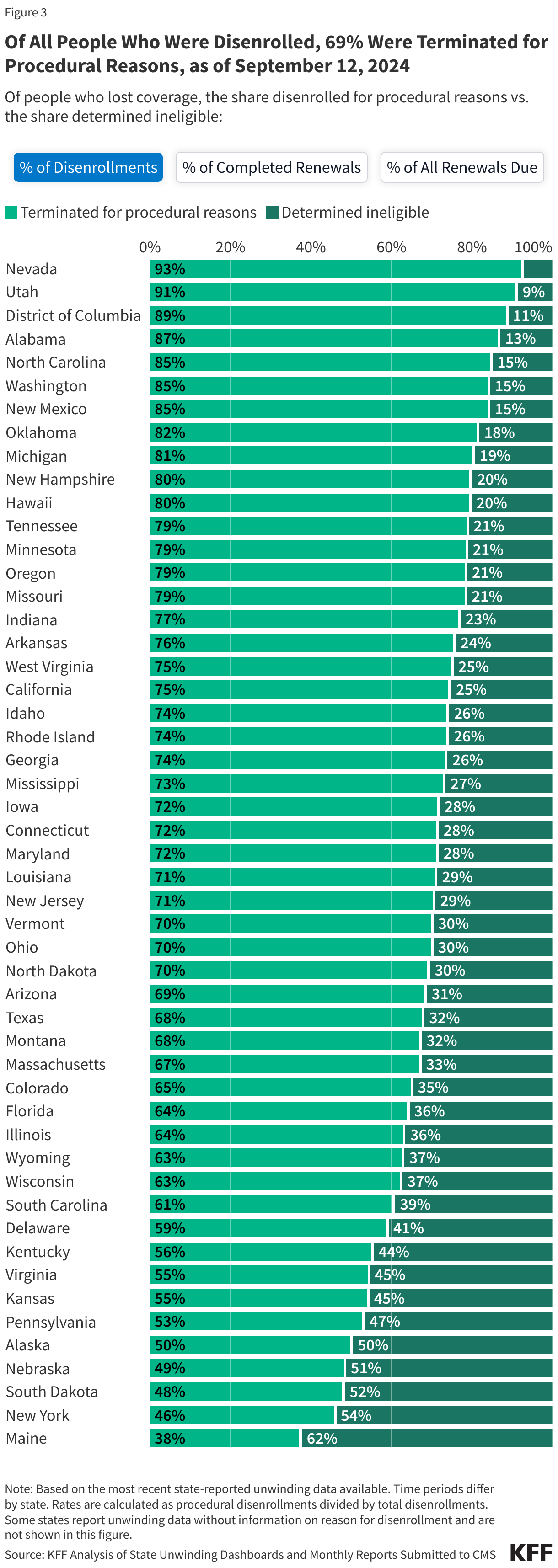
Procedural Disenrollment: A Crisis of Process
One of the most concerning findings from the 2024 data was the prevalence of "procedural disenrollment." Of the roughly 25 million people removed from the rolls by late 2024, 69% were terminated for procedural reasons. This means these individuals lost coverage not because they were necessarily ineligible, but because they failed to complete the administrative paperwork required to renew their status—often due to notice delivery issues, lack of language access, or administrative backlogs.
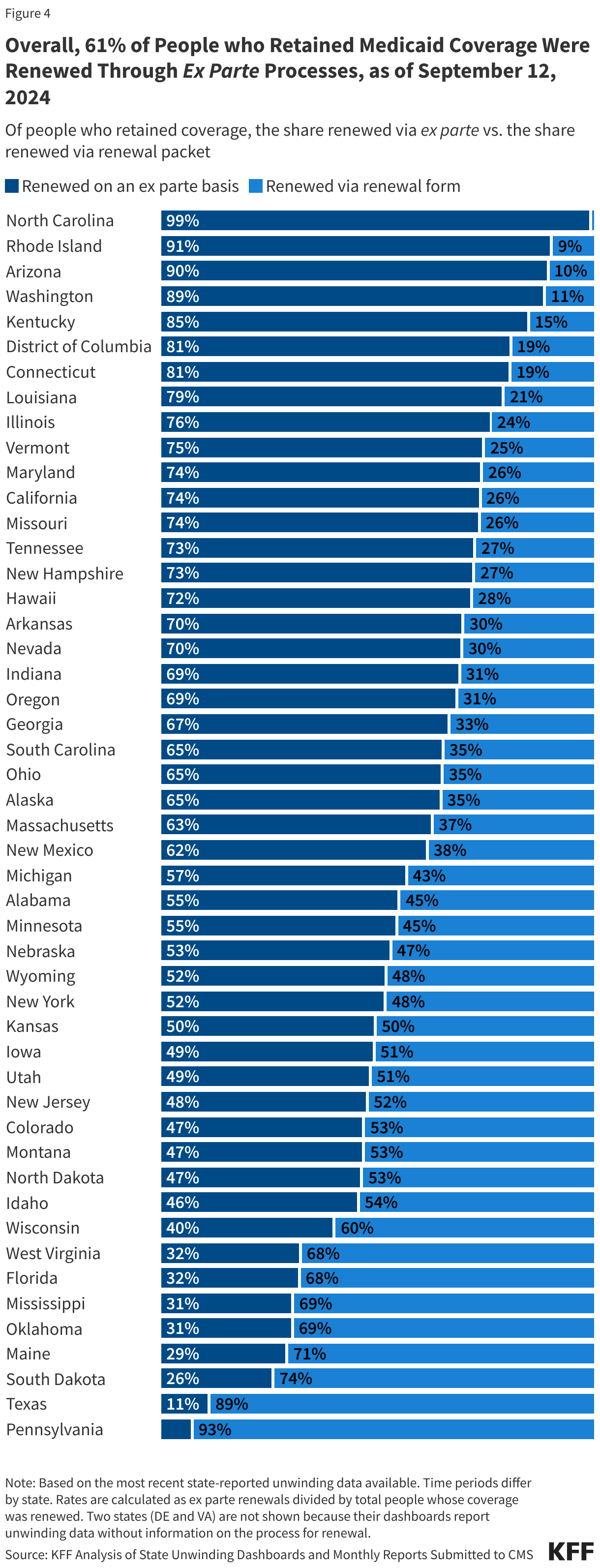
The Success of Ex Parte Renewals
Conversely, data highlighted the effectiveness of "ex parte" renewals—a process where the state automatically renews coverage using existing electronic data. Overall, 61% of individuals who successfully retained coverage were renewed through these automated systems. This disparity suggests that when states invest in automated, data-driven systems, they achieve higher rates of coverage continuity compared to systems that rely on manual beneficiary reporting.
Official Responses and Policy Implications
The implementation of the 2025 reconciliation law has drawn sharp criticism from health policy researchers and advocacy groups. The primary concern is that the new work and reporting requirements will inadvertently create a "coverage gap" for vulnerable populations.
The Impact of Work Requirements
Proponents of the 2025 law argue that work requirements promote self-sufficiency and align with the fiscal goals of the budget reconciliation process. However, the KFF (Kaiser Family Foundation) and other research entities warn that these requirements will likely act as a barrier to care rather than a gateway to employment. Many enrollees who are technically eligible for coverage may lose it simply because they cannot navigate the rigorous monthly reporting requirements, mirroring the procedural disenrollment issues observed during the unwinding.
Restrictions on Immigrant Eligibility
The scheduled restrictions on immigrant eligibility for October 2026 represent a deliberate policy choice to limit the scope of the program. Analysts suggest that this will likely lead to an increase in uncompensated care costs at the hospital level, as individuals who are no longer eligible for Medicaid or CHIP may delay seeking preventative care, eventually presenting at emergency departments with more advanced, expensive-to-treat conditions.
Long-term Economic Consequences
The Congressional Budget Office (CBO) and other independent observers have projected that the 2025 law will significantly reduce enrollment over the next decade. While this will result in lower federal and state spending on Medicaid, the implications for public health are profound. The reduction in coverage is expected to exacerbate existing health disparities, particularly in rural and low-income urban communities where Medicaid serves as the primary safety net.
Analyzing the Future of Medicaid Watch
The "Medicaid Watch" initiative, which tracks these policy shifts, remains a vital resource for understanding the ground-level impact of these legislative changes. As the deadline for the January 2027 work requirements approaches, the focus is shifting toward state-level implementation.
Several states have signaled their intent to implement these requirements early. This creates a fragmented national landscape where an individual’s access to healthcare may depend heavily on their state of residence. The variation in administrative capacity between states—some with robust, modernized eligibility systems and others with legacy paper-based systems—will likely result in a highly inconsistent rollout of the new mandates.
Conclusion: A System at a Crossroads
The decade spanning from 2014 to 2025 serves as a masterclass in the volatility of public health policy. Medicaid has evolved from a program that expanded to meet the needs of the working poor to a system currently navigating a period of intentional administrative contraction.
The data through early 2026 paints a clear picture: enrollment is sensitive not just to economic conditions, but to the administrative burdens placed upon the most vulnerable citizens. As the 2025 Reconciliation Law takes full effect over the coming years, the primary challenge for the American healthcare system will be balancing fiscal responsibility with the fundamental goal of ensuring health equity for millions of low-income adults and children. Whether the system can modernize its renewal processes sufficiently to avoid the mass procedural disenrollments of the past remains the defining question for the remainder of the decade.
For researchers and stakeholders, the data presented in this report, including the archived figures from the unwinding period, are available through the CMS Performance Indicator Project and the KFF state-level tracking tools. Questions regarding specific methodology or updates to these trackers can be directed to the KFF research team.