The landscape of modern pharmacology is currently witnessing a profound renaissance. Once relegated to the margins of drug design due to fears of systemic toxicity, covalent drugs have re-emerged as a cornerstone of precision medicine. From the early, serendipitous success of aspirin to the highly engineered, targeted covalent inhibitors (TCIs) of the 21st century, these compounds have proven capable of tackling "undruggable" disease targets. However, their unique mechanism—the formation of a permanent chemical bond with a biological target—requires a radical departure from traditional pharmacokinetic (PK) paradigms.
The Evolution of Covalent Therapeutics: From Serendipity to Precision
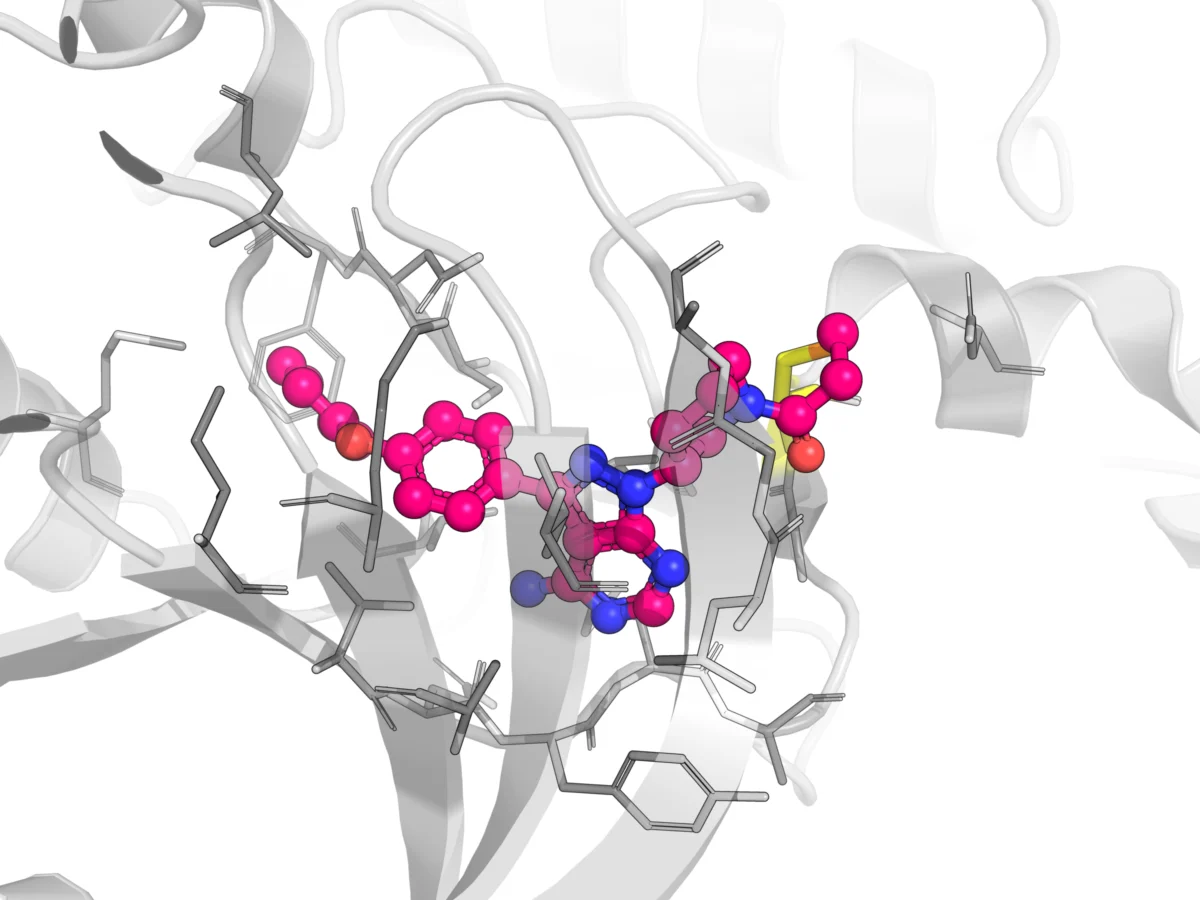
Covalent drugs function by forming a stable chemical bond with a specific amino acid residue, typically a cysteine, within the active site of an enzyme or receptor. This permanent attachment effectively deactivates the target, providing a level of potency and duration of action that reversible, non-covalent inhibitors often struggle to achieve.
A Historical Perspective
The history of covalent medicine is a tale of two eras. The first era, beginning with the 1899 approval of aspirin, was defined by clinical efficacy that outpaced mechanistic understanding. It took seven decades to fully elucidate how aspirin covalently modifies cyclooxygenase (COX). Similarly, the mechanism by which penicillin binds to bacterial transpeptidase—a discovery that saved millions of lives—remained opaque for over 50 years after the drug’s clinical introduction.
The "No-Go" Era and the Return to Electrophiles
By the mid-20th century, the field hit a wall. Early covalent drugs utilized highly reactive electrophiles that lacked target specificity. These "promiscuous" molecules would bind indiscriminately to DNA, lipids, and off-target proteins, leading to catastrophic toxicities. The medical community’s association of electrophiles with toxic agents like mustard gas led to a decades-long abandonment of covalent chemistry in favor of reversible, non-covalent drug development.
The current renaissance is built upon the refinement of "soft" electrophiles. Modern medicinal chemistry now utilizes warheads like acrylamides and nitriles, which are engineered for moderate reactivity. By carefully tuning the electrophilicity of these warheads, developers can ensure the drug reacts only with a specific, nucleophilic target residue, effectively neutralizing the risk of off-target cellular damage. Today, more than 110 covalent drugs are approved, including modern oncology breakthroughs like osimertinib, which has fundamentally altered the prognosis for certain lung cancer patients.
Pharmacokinetic Paradoxes: Why Traditional Metrics Fail
For standard small-molecule drugs, the relationship between plasma concentration and therapeutic effect is relatively linear. As the drug is cleared from the bloodstream, its efficacy wanes. Covalent drugs, however, follow a different set of rules. Because they form a permanent bond, the pharmacodynamic (PD) effect is often independent of the plasma concentration.
The Decoupling of PK and PD
The most significant challenge for developers is the decoupling of PK/PD. In traditional drug discovery, maintaining a steady-state plasma concentration is the gold standard. For a covalent inhibitor, the duration of action is governed not by the drug’s plasma half-life, but by the turnover rate of the target protein.
As seen in studies of the BTK inhibitor CC-292, plasma levels may drop below detectable limits within 24 hours, yet the therapeutic effect persists because the target enzyme has not yet been resynthesized by the cell. Consequently, drug developers must shift their focus from maintaining continuous plasma exposure to prioritizing high, rapid target engagement (Cmax-driven).
Navigating the Complexity: Off-Target Reactivity and Clearance
While covalent binding to the target is the goal, the reality of systemic circulation introduces inevitable off-target interactions. Understanding these is vital for safety profiles.
Protein Adduction and Distribution
Covalent drugs can form stable adducts with human serum albumin (HSA) and other tissue proteins. While high levels of protein binding are often viewed as a negative in traditional PK, for covalent drugs, this is a nuanced factor. Binding to HSA can reduce the concentration of the "free" drug in the plasma, acting as a reservoir that influences both the drug’s distribution and its eventual clearance. Developers must learn to distinguish between harmless off-target binding and meaningful, toxicity-inducing reactivity.
Clearance Mechanisms and Metabolic Pathways
The clearance of covalent inhibitors often involves specialized pathways, such as conjugation with glutathione (GSH) or cysteine. For instance, the FGFR inhibitor Futibatinib undergoes extensive metabolism, with various GSH, cysteine, and glucuronide conjugates appearing in the bloodstream.
- Strategic Recommendation: Developers should implement rigorous screening for non-enzymatic and GST-mediated reactivity early in the discovery phase. Utilizing recombinant GST isoforms and advanced hepatocyte models allows for a more accurate assessment of how genetic polymorphisms might impact a patient’s ability to clear these adducts, thereby reducing the risk of unexpected hepatotoxicity.
Time-Dependent Inhibition (TDI) of CYP450
A persistent risk for covalent drug candidates is the potential for time-dependent inhibition (TDI) of cytochrome P450 (CYP) enzymes. Because these drugs are inherently designed to bind to proteins, they are predisposed to "accidentally" binding to the active sites of CYP enzymes. Research indicates that many covalent drugs exhibit TDI across various CYP isoforms, creating significant risks for drug-drug interactions (DDIs). Early kinetic characterization—specifically measuring the $KI$ and $kinact$ values—is essential for predicting clinical risk and guiding necessary structural optimizations before a molecule reaches the clinic.
Implications for Future Drug Development
The shift toward covalent inhibitors represents a move toward more "permanent" therapeutic solutions. However, the regulatory and development burden is higher than that of traditional drugs.
A New Screening Paradigm
The industry is moving toward a more robust screening paradigm. As Dr. Qigan Cheng of WuXi AppTec notes, successful covalent programs must demonstrate "deliberate, selective chemistry." This requires:
- Kinetic Profiling: Early assessment of reaction kinetics to ensure the warhead is optimized for the specific target.
- Mechanistic Modeling: Moving away from simple PK modeling toward complex PK/PD models that account for target resynthesis rates.
- Safety-First Design: Rigorous testing for off-target adduct formation to ensure that the drug’s "warhead" is only triggered by the intended biological target.
The Road Ahead
The success of covalent drugs in oncology and infectious disease is only the beginning. As we refine our ability to predict the behavior of soft electrophiles and better manage the unique clearance pathways of these molecules, the scope of "druggable" targets will continue to expand.
For the modern development team, the challenge lies in the marriage of chemistry and systems biology. By understanding that the drug is not merely a passenger in the bloodstream but an active, reactive participant in cellular metabolism, researchers can design therapies that are both highly potent and exquisitely safe. The future of medicine lies in our ability to guide these powerful chemical tools with the precision of a scalpel, ensuring that the covalent bond—once the source of toxicity—becomes the hallmark of modern, curative therapy.
Summary of Key Considerations for Developers
- Target Occupancy is King: Do not optimize for plasma half-life. Focus on achieving rapid, maximum target engagement (Cmax).
- Quantify Reactivity Early: Use hepatocyte systems to rank the electrophilicity of your warheads and minimize the potential for off-target protein adduction.
- Monitor DDI Potential: Given the tendency for covalent drugs to act as TDIs, incorporate CYP inhibition studies early to guide dosing and minimize the risk of clinical drug-drug interactions.
- Leverage Mechanistic Models: Use target turnover data to determine dosing frequency rather than relying on standard PK-based dosing schedules.
By embracing these specialized pharmacokinetic strategies, the biopharmaceutical industry can continue to unlock the immense potential of covalent inhibition, providing new hope for patients facing diseases that were, until recently, considered beyond our reach.