

Introduction
The landscape of the American social safety net underwent a seismic shift between 2023 and 2024, a period defined by the massive administrative undertaking known as the "Medicaid Unwinding." Following three years of unprecedented federal protections that prohibited states from disenrolling individuals from Medicaid and the Children’s Health Insurance Program (CHIP), the expiration of the continuous enrollment provision in early 2023 forced a nationwide redetermination process. This report examines the data-driven consequences of this transition, exploring how nearly 94 million enrollees—a record high achieved during the pandemic—faced a complex, state-led renewal process that permanently altered the reach of public health coverage in the United States.
Main Facts: The End of an Era
The COVID-19 pandemic triggered the Families First Coronavirus Response Act, which included a "continuous enrollment" provision. This policy ensured that Medicaid enrollees remained covered regardless of changes in their eligibility status, provided states maintained these rolls in exchange for enhanced federal funding.
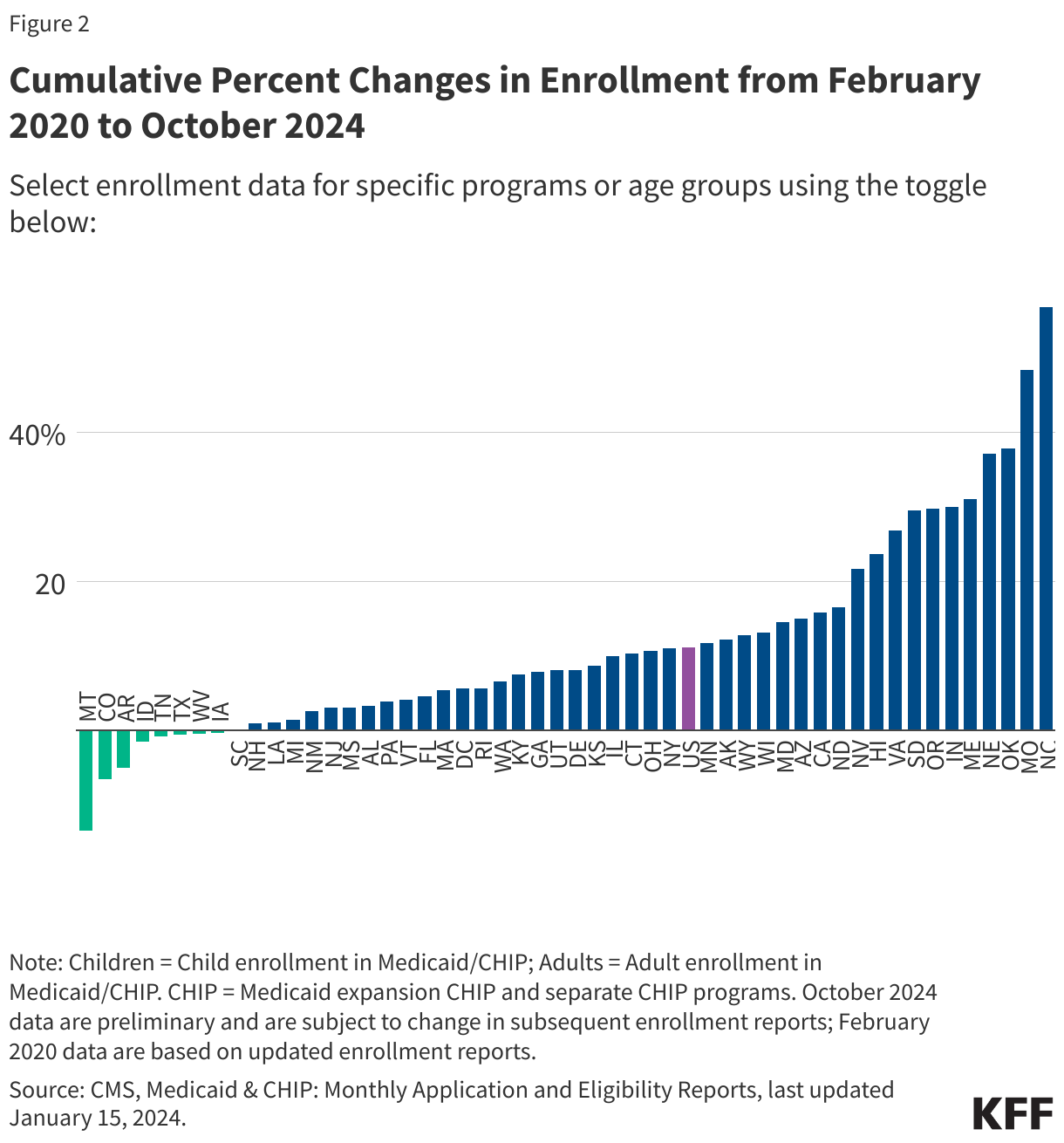
By the time this provision lapsed on March 31, 2023, the system had grown to accommodate 94 million Americans. The subsequent "unwinding" was not a singular event but a staggered, state-by-state process that took approximately 18 months to conclude. As of the final reporting cycles in August and September 2024, the data reveal a landscape of significant disenrollment, high procedural terminations, and a reliance on "ex parte" (automated) renewal systems.
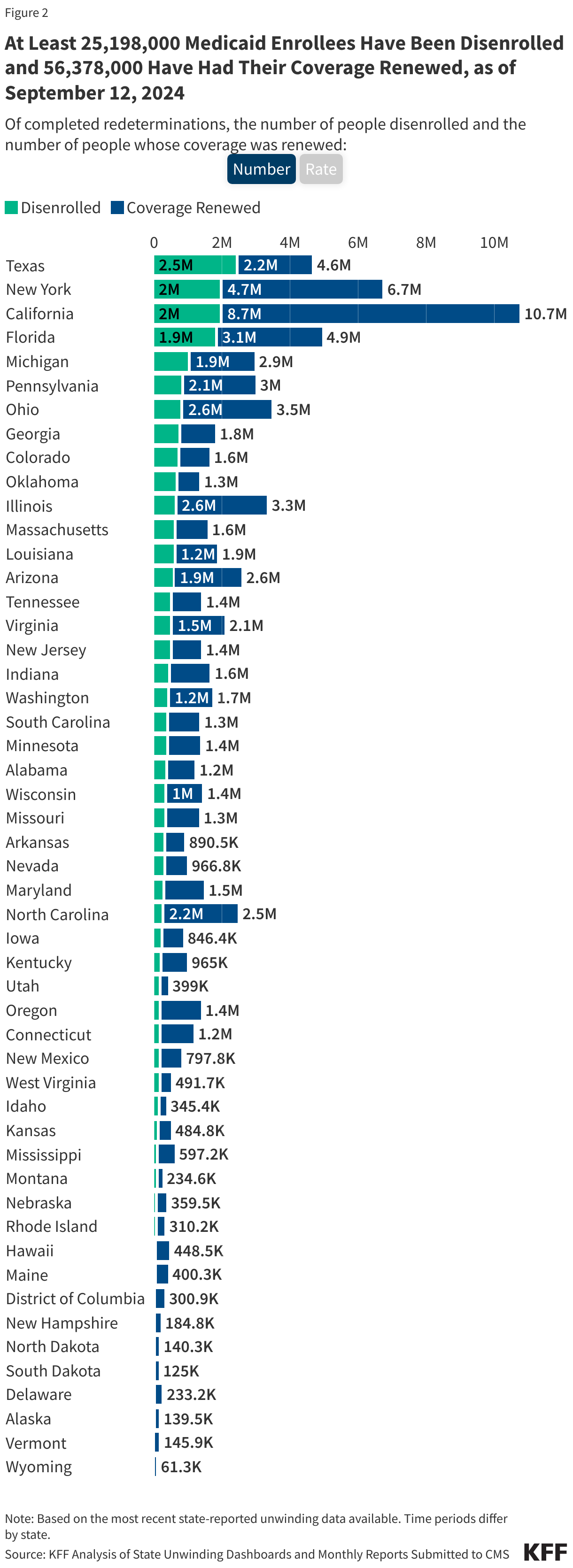
Key takeaways from the concluded unwinding period include:
- Mass Disenrollment: At least 25.19 million individuals lost their Medicaid or CHIP coverage during the unwinding.
- Coverage Retention: Over 56 million people successfully navigated the renewal process and maintained their status.
- The Procedural Hurdle: Approximately 69% of all disenrollments were categorized as "procedural," meaning coverage was lost not necessarily because the individual was ineligible, but because they failed to complete the administrative requirements of the renewal process.
Chronology: From Pandemic Protection to Redetermination
The timeline of the Medicaid Unwinding is essential for understanding the scale of the transition.
The Pandemic Baseline (February 2020 – March 2023)
Prior to the pandemic, Medicaid rolls fluctuated based on economic conditions. The onset of COVID-19 in February 2020 served as the baseline. The federal continuous enrollment provision effectively froze the system, leading to a steady climb in enrollment as economic uncertainty spiked and federal mandates prevented coverage losses.
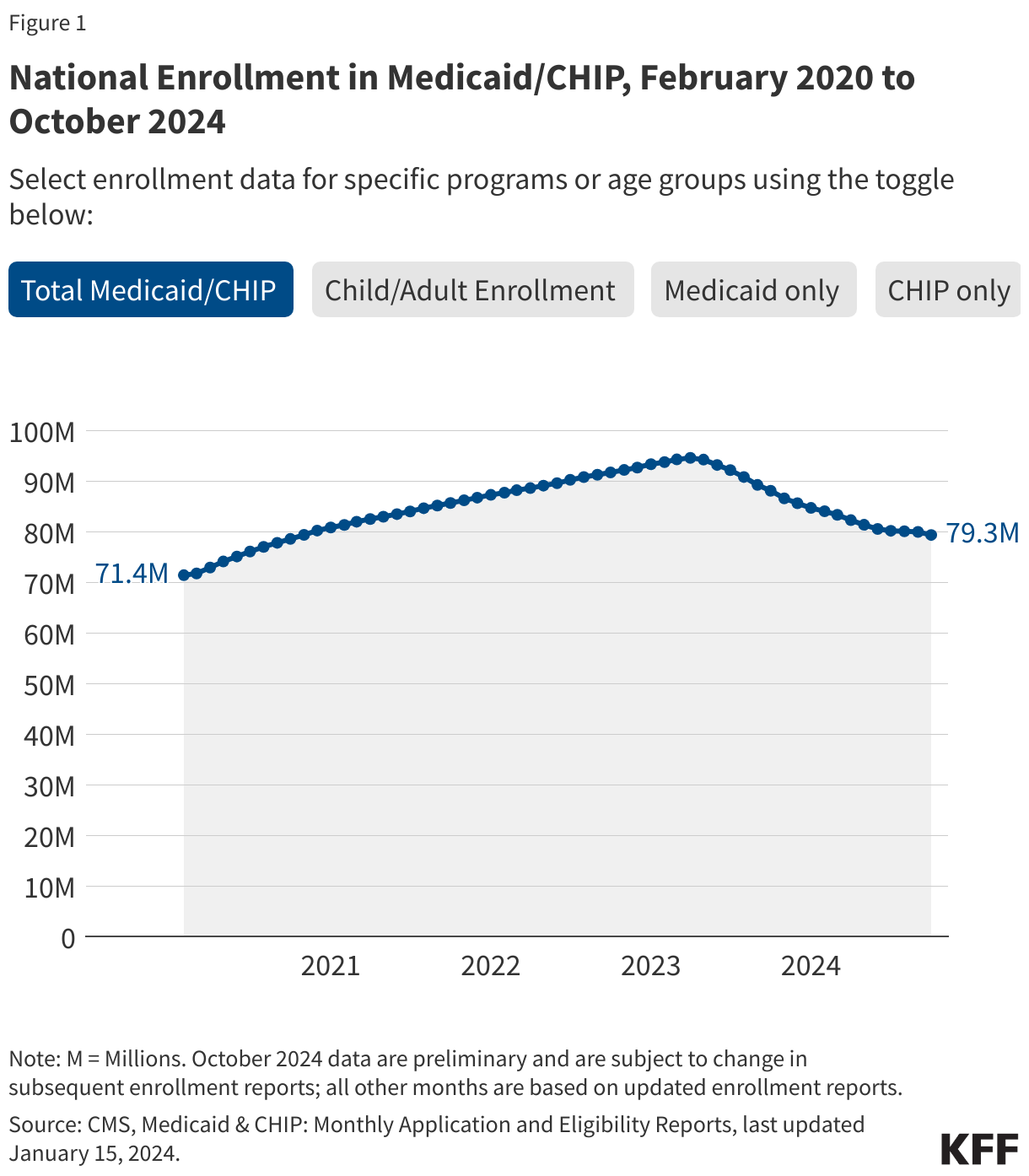
The Unwinding Begins (April 2023 – August 2024)
States were granted the authority to begin disenrolling ineligible enrollees starting April 1, 2023. However, the rollout was not uniform. While many states initiated their processes immediately, some delayed action until May, June, or July 2023. The 12-month renewal window meant that most states had completed their initial redetermination cycles by the late summer of 2024.
The Post-Unwinding Era (September 2024 – Present)
As of September 12, 2024, the federal government and state agencies ceased the active "unwinding" reporting metrics. The system has now shifted back to "business as usual" operations, where states must conduct annual renewals under standard federal regulations. The data collected during this period remains the most comprehensive record of how states manage the delicate balance between program integrity and access to care.
Supporting Data: Dissecting the Outcomes
The sheer scale of the administrative data provided by the Centers for Medicare & Medicaid Services (CMS) allows for a granular look at the efficacy of state processes.
Renewal Success and the "Ex Parte" Process
One of the most significant metrics identified in the analysis is the reliance on ex parte renewals. This is an automated system where states use existing data—such as tax records or SNAP enrollment—to verify eligibility without requiring the enrollee to fill out a new form. Data indicates that 61% of individuals who retained their coverage did so through these automated processes. This statistic highlights the critical role of state-level digital infrastructure; states with robust data-matching capabilities saw significantly higher retention rates than those relying on manual, paper-based renewals.
The Procedural Disenrollment Crisis
The most concerning trend remains the high rate of procedural disenrollments. When an individual is terminated for "procedural" reasons, it often indicates a breakdown in communication: the state sent a renewal notice to an outdated address, the enrollee did not understand the form, or they were unable to navigate the state’s portal in time. With 69% of those removed from the rolls falling into this category, the data suggests that millions of people may have been disenrolled despite still meeting the income and eligibility requirements for the program.
Official Responses and Policy Implications
The "unwinding" sparked intense debate among health policy experts, state governors, and federal regulators.

Federal Oversight
CMS, through the Performance Indicator Project, required states to submit monthly reports to monitor for "red flags"—such as long call-center wait times or high rates of child disenrollment. Federal officials consistently urged states to prioritize automated renewals and conduct robust outreach, though the variability in state implementation led to a fragmented experience for enrollees.
State-Level Variability
State approaches varied wildly. Some states, like California and New York, implemented aggressive public awareness campaigns and extended grace periods for paperwork. Others, facing budget pressures or political pressure to shrink the size of the Medicaid rolls, utilized more stringent verification processes. The archived data serves as a permanent record of these choices, allowing researchers to compare the long-term health outcomes of states that pursued aggressive disenrollment against those that prioritized continuous coverage.
Implications: The Future of Public Health Coverage
The conclusion of the unwinding does not mean the end of the challenge. The implications for the U.S. healthcare system are profound and multi-faceted.
The "Coverage Gap" and Private Market Transitions
Many individuals who were disenrolled from Medicaid transitioned into employer-sponsored insurance or the Affordable Care Act (ACA) marketplace. However, for those who slipped through the cracks, the loss of coverage represents a direct barrier to primary care, prescription medications, and chronic disease management.
Long-term Administrative Reform
The "procedural" disaster of the last two years has forced a national conversation regarding administrative burdens in public assistance. There is a growing bipartisan push to modernize state systems, specifically by investing in better data-sharing technologies that can reduce the burden on families. The lessons learned from the unwinding are likely to shape future Medicaid regulations, with an emphasis on "auto-enrollment" and "auto-renewal" as the standard for the future.
Impact on Vulnerable Populations
Children and low-income families were disproportionately impacted by the unwinding process. As Medicaid serves as the primary insurer for a large percentage of the nation’s children, the administrative hurdles they faced during the transition have raised concerns about potential gaps in childhood vaccination, wellness checks, and early childhood development support. Policymakers are now tasked with assessing the "unwinding" in the context of broader health equity goals.
Conclusion: A Data-Driven Legacy
The Medicaid Unwinding of 2023-2024 stands as the largest administrative disruption to health coverage in modern American history. By examining the 94-million-enrollee peak and the subsequent, often-volatile process of returning to pre-pandemic rules, we gain a clearer understanding of the fragility of the social safety net.
While the data reporting has largely ceased, the impact remains. Millions of Americans are now in a post-unwinding environment, navigating a mix of private, public, or, in some cases, no insurance at all. The lessons from this period—specifically the necessity of automated, efficient renewal systems—will remain the focal point for health policy advocates, government officials, and healthcare providers for years to come. The goal moving forward is not merely to "manage" enrollment but to ensure that the administrative processes meant to protect the integrity of the program do not become the very barrier that denies citizens their right to health.
For researchers and citizens seeking to delve deeper into specific state-level metrics, the archives provided by KFF and CMS remain the primary source of truth. As the nation moves forward, these figures will continue to serve as the definitive benchmark for measuring the accessibility and efficacy of Medicaid in a post-pandemic world.






