
More than a decade after the passage of the Affordable Care Act (ACA), the landscape of American public health remains sharply divided by a policy decision that has become a litmus test for state-level governance: Medicaid expansion. By extending health coverage to nearly all low-income adults with household incomes up to 138% of the Federal Poverty Level (FPL)—equating to an annual income of $21,597 for an individual in 2025—the ACA sought to close the "coverage gap" that left millions of Americans without access to affordable healthcare. Today, as 41 states and the District of Columbia have embraced this expansion, the 10 states that remain holdouts represent a significant, ongoing debate regarding federal mandates, fiscal responsibility, and the social contract of healthcare.
The Mechanics of Expansion: A Federal-State Partnership
At its core, the Medicaid expansion was designed as a federal-state partnership, incentivized by a generous federal matching rate. Under the ACA, the federal government covers a significant majority—and for the expansion population, a vastly enhanced portion—of the costs incurred by states that choose to participate.
The threshold of 138% of the FPL was established to ensure that those who earn too much to qualify for traditional Medicaid but too little to afford private insurance premiums on the open market could access comprehensive, subsidized health coverage. For millions of working-class Americans, this provision has served as a critical safety net, providing access to primary care, chronic disease management, and preventative services that were previously out of reach.
A Chronological Evolution: From Supreme Court Ruling to Present Day
The history of Medicaid expansion is one of unexpected legal turns and persistent political friction.
2010–2012: The Mandate and the Challenge
When the ACA was signed into law in 2010, the Medicaid expansion was initially written as a mandatory requirement for all states. However, the 2012 Supreme Court ruling in National Federation of Independent Business v. Sebelius fundamentally altered the policy’s trajectory. While the Court upheld the ACA, it ruled that the federal government could not coerce states into expanding their Medicaid programs by threatening to withhold their entire existing Medicaid funding. This effectively rendered the expansion an "optional" choice for states.
2014: The Rollout
On January 1, 2014, the first wave of states implemented the expansion. The initial response was characterized by a distinct partisan divide, with Democratic-led states largely embracing the influx of federal dollars, while many Republican-led states opted out, citing concerns over long-term fiscal sustainability and the philosophical objection to expanding a government-run entitlement program.
2015–2020: The Ballot Initiative Era
As the policy debate stagnated in many state legislatures, advocates turned to the ballot box. Between 2017 and 2020, states like Maine, Idaho, Nebraska, and Utah saw voters bypass their recalcitrant legislatures to approve Medicaid expansion via direct ballot initiatives. This period marked a pivotal shift in the discourse, proving that Medicaid expansion held broad bipartisan popularity among the general electorate, even in traditionally conservative states.
2021–Present: The Final Push
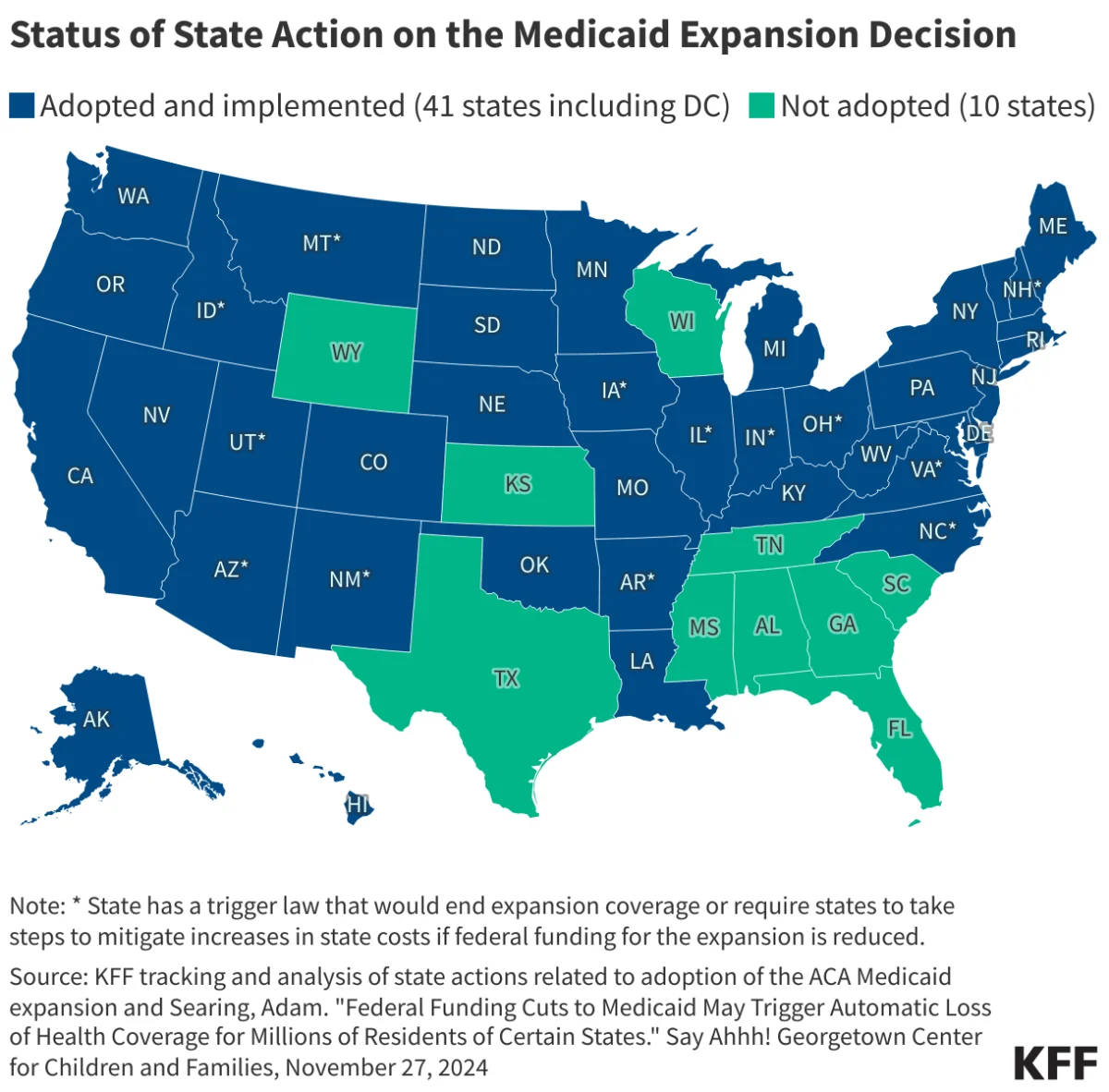
Recent years have seen further momentum, with states like North Carolina and South Dakota adopting expansion. However, the remaining 10 states—primarily clustered in the South—continue to hold firm, creating a stark visual divide on the national map. According to current tracking by KFF, the status of these holdout states remains a focal point for health policy analysts and political observers alike.
Supporting Data: The Cost of Disparity
The data surrounding Medicaid expansion paints a compelling, if complex, picture of the policy’s impact. KFF’s continuous tracking provides the most granular view of state-level adoption.
The enhanced Federal Medical Assistance Percentage (FMAP) provided to states for the expansion population is a central pillar of the program. For many states, the influx of federal funds has not only covered the costs of the new enrollees but has also provided a boost to state economies. Hospitals in expansion states, particularly those in rural areas, have seen a marked decrease in uncompensated care costs. Conversely, in non-expansion states, rural hospitals continue to face existential threats, with many closing their doors due to the financial strain of treating a high volume of uninsured, low-income patients.
Furthermore, longitudinal studies have shown that expansion states experience better health outcomes, including earlier cancer diagnoses, improved management of diabetes and hypertension, and lower maternal mortality rates. The financial burden on families in non-expansion states, by contrast, is often higher, as they are forced to rely on emergency rooms for routine care, a practice that is both inefficient and expensive for the healthcare system as a whole.
Official Responses: The Philosophical and Fiscal Debate
The divide over Medicaid expansion is rarely about the mechanics of the policy and almost always about the underlying philosophy of government.
The Pro-Expansion Argument
Supporters, including the American Medical Association, hospital associations, and various advocacy groups, argue that Medicaid expansion is a moral and economic imperative. They contend that the "enhanced FMAP" makes the policy essentially "too good to pass up." From their perspective, the federal government is providing states with billions of dollars that are currently being diverted to other states. They point to the "coverage gap"—individuals who earn too little to qualify for ACA marketplace subsidies but too much to qualify for non-expansion Medicaid—as a failure of the state to protect its most vulnerable citizens.
The Anti-Expansion Argument
Opponents, often citing the fiscal autonomy of the state, argue that the expansion represents an unsustainable expansion of the welfare state. Critics frequently highlight the "long-term risk" that the federal government might eventually reduce its matching rate, leaving states on the hook for a massive, permanent liability. Additionally, some conservative policymakers argue that Medicaid is fundamentally broken, citing issues with provider access and quality of care, and argue that state-based innovations—rather than a "one-size-fits-all" federal mandate—are the better path forward for healthcare reform.
Implications for the Future of American Healthcare
The implications of the remaining 10 states refusing to expand Medicaid are profound.
The Coverage Gap
The primary implication is the persistence of the coverage gap. Hundreds of thousands of adults in the South remain in a state of health-coverage limbo. They are often working in low-wage sectors—retail, hospitality, or agriculture—yet they remain ineligible for any meaningful financial assistance for health insurance. This gap is not merely a statistical anomaly; it is a lived reality for families who must decide between buying groceries and filling a prescription.
Fiscal Federalism
The ongoing stalemate serves as a case study in the complexities of American fiscal federalism. The ACA was designed to create a uniform national standard, yet the Supreme Court’s 2012 intervention effectively allowed for a "fragmented" system. This fragmentation has created a "health insurance zip code lottery," where the quality of one’s access to care is determined entirely by the state of residence.
Economic and Health Equity
Looking forward, the health and economic disparities between expansion and non-expansion states are projected to widen. As medical technology advances and the cost of care continues to rise, the lack of a robust, state-supported safety net will likely result in deeper health inequities. Public health experts argue that without universal adoption, the United States will continue to struggle with a bifurcated healthcare system that fails to provide basic protection to its workforce.
Conclusion
The Medicaid expansion under the Affordable Care Act remains one of the most consequential public health policies in modern American history. With 41 states having taken the step toward broader coverage, the policy has transformed the lives of millions. Yet, the 10 states that remain outside the expansion framework serve as a stark reminder of the deep political and ideological fissures that continue to define the American healthcare debate.
Whether these final states will eventually move toward adoption remains a subject of intense speculation. What is certain, however, is that as long as the map remains divided, the conversation surrounding the moral, fiscal, and social obligations of the state to its citizens will remain at the forefront of the national consciousness. For the individuals living in the shadow of this divide, the wait for a resolution is not a matter of political theory, but a matter of daily health and survival.






