Executive Summary
In an era where mental health awareness has reached a critical zenith, the economic reality of accessing care remains a daunting hurdle for millions of Americans. A comprehensive analysis released by the Peterson-KFF Health System Tracker, utilizing 2023 data from the Merative MarketScan Commercial Claims Database, has unveiled the significant footprint of mental health and substance use disorders (SUD) within the U.S. commercial insurance landscape.
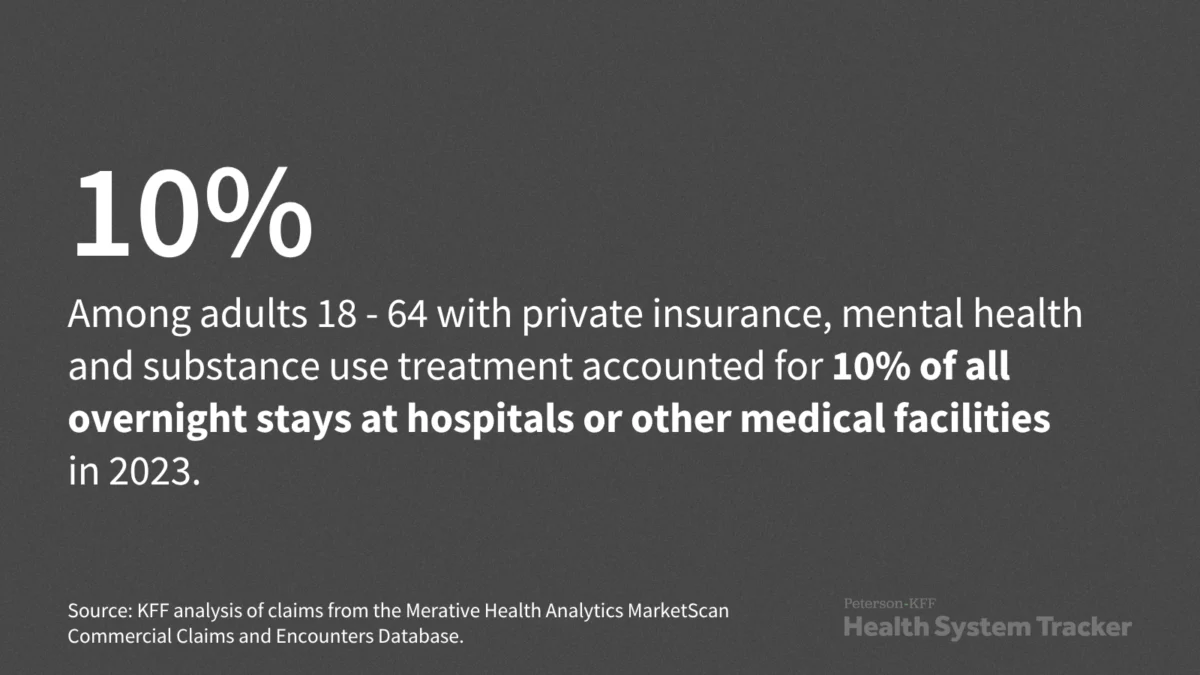
The report highlights that inpatient treatment for these conditions accounted for 10% of all commercial inpatient stays in 2023, translating to a rate of 32 per 10,000 enrollees. With average costs hovering between $15,500 and $15,900 per admission, the financial strain on both insurance systems and individual households is profound. This article examines the trajectory of these costs, the implications for policy, and the systemic challenges inherent in treating behavioral health within the current commercial insurance framework.
Main Facts: The Economic Scale of Behavioral Health
The Peterson-KFF analysis serves as a definitive snapshot of the U.S. behavioral health crisis. By analyzing claims data, researchers were able to quantify not just the volume of care, but the direct financial impact on the private insurance sector.
Key takeaways from the 2023 dataset include:
- Volume of Care: Mental health and substance use treatments comprised one-tenth of all commercial inpatient admissions.
- Cost Disparity: A mental health-related admission carries an average mean total cost of $15,900. Substance use admissions are marginally lower but remain substantial, averaging $15,500 per stay.
- The Burden of Costs: These figures represent the total cost, an aggregate of both the insurer’s contribution and the patient’s out-of-pocket financial liability.
- Demographics of Utilization: With a frequency of 32 per 10,000 enrollees, the data underscores that these treatments are not rare occurrences but are integrated into the standard utilization patterns of the American workforce covered by commercial plans.
Chronology: The Evolution of Behavioral Health Treatment
To understand the significance of these 2023 figures, one must look at the historical context of behavioral health treatment in the United States.
The Pre-Parity Era (Pre-2008)
Historically, mental health treatment was relegated to a second-tier status within health insurance. Coverage was often capped, and benefits were significantly less generous than those for physical health conditions. The "Mental Health Parity and Addiction Equity Act" (MHPAEA) of 2008 was a landmark legislative effort designed to force insurers to cover mental health services with the same level of coverage as medical and surgical procedures.
The Pandemic Shift (2020–2022)
The COVID-19 pandemic served as a massive accelerator for behavioral health utilization. Increased social isolation, economic anxiety, and the rapid expansion of telehealth services brought mental health into the public consciousness. During this period, the surge in demand for inpatient services began to climb, as acute mental health crises—particularly among adolescents and young adults—reached historic highs.
The 2023 Data Baseline
The 2023 data provided by Peterson-KFF represents a "new normal." It captures a post-pandemic healthcare environment where the infrastructure for mental health care has been tested to its limits. By 2023, the backlog of care, coupled with a growing willingness to seek professional treatment, resulted in the stabilized 10% utilization rate reported by the analysis.
Supporting Data: Deconstructing the Costs
Understanding the $15,000+ price tag for an inpatient stay requires an examination of the cost components. Unlike elective surgeries, which are often scheduled and predictable, behavioral health admissions are frequently emergency-driven.
Inpatient Stays vs. Outpatient Care
While the report focuses on inpatient stays, it is vital to note that these figures only account for the most severe cases. Inpatient treatment is generally reserved for patients at risk of self-harm, severe psychosis, or acute withdrawal symptoms from substance use. The high cost reflects the intensity of 24-hour medical supervision, nursing care, and specialized psychiatric oversight required in these settings.
Out-of-Pocket Realities
For the average American, a $15,000 bill is catastrophic, even with insurance. The analysis highlights that the total cost is split between the insurer and the patient. Depending on the patient’s specific plan—deductibles, copays, and coinsurance—an inpatient stay can result in thousands of dollars in debt. Even with "parity" laws in place, high-deductible health plans (HDHPs) frequently shift a larger percentage of the cost to the patient, potentially creating a barrier to entry that prevents individuals from seeking the care they need until they reach a point of crisis.
Official Responses and Industry Implications
The KFF analysis has resonated throughout the healthcare policy community, prompting responses from advocates, insurance lobbyists, and federal regulators.
The Advocacy Perspective
Mental health advocacy groups, such as NAMI (National Alliance on Mental Illness), argue that these costs are evidence of a system that still treats mental health as a secondary priority. "While we have parity laws on the books, the implementation at the claims level remains inconsistent," noted one policy advisor. Advocacy groups point to "network adequacy" as the true culprit—if patients cannot find in-network psychiatric care, they are forced into expensive out-of-network settings or emergency rooms, which balloon costs.
The Insurer Perspective
Conversely, health insurance representatives emphasize the rising cost of medical supplies, hospital staffing, and the specialized labor required for mental health wards. They argue that the high cost of inpatient stays is a function of a shortage of mental health professionals. If there were more outpatient community-based resources, they contend, fewer patients would reach the acute stage requiring expensive hospitalization.
Implications: The Road Ahead
The findings from the Peterson-KFF Health System Tracker present several long-term implications for the U.S. healthcare system:
1. The Need for Proactive Care
If 10% of all commercial stays are dedicated to behavioral health, the system is clearly over-reliant on the most expensive form of care: the hospital bed. Shifting resources toward early intervention and robust outpatient networks is not just a moral imperative but an economic necessity.
2. Regulatory Enforcement
The 2023 data suggests that the Department of Labor and the Centers for Medicare & Medicaid Services (CMS) must continue to rigorously audit insurance plans to ensure that their "non-quantitative treatment limitations" (NQTLs)—such as prior authorization requirements—are not unfairly obstructing access to care.
3. The Impact on Workforce Productivity
For commercial insurers, the primary customer is the employer. The data showing high inpatient costs highlights the "hidden" cost of behavioral health to businesses. Absenteeism, reduced productivity, and long-term disability claims related to untreated mental health conditions cost the U.S. economy billions annually. This makes investing in mental health benefits an increasingly attractive strategy for corporate retention and operational stability.
4. Addressing Substance Use Treatment
The proximity of costs between mental health ($15,900) and substance use ($15,500) admissions highlights that the addiction epidemic remains a major driver of healthcare spending. The data suggests that as long as the underlying causes of substance use remain inadequately addressed in the primary care setting, the reliance on high-cost, acute-care inpatient facilities will persist.
Conclusion
The Peterson-KFF analysis is more than a collection of statistics; it is a diagnostic tool for the American healthcare system. By illuminating the financial reality of mental health and substance use treatment, it forces a conversation about the effectiveness of current insurance models and the adequacy of the behavioral health infrastructure.
As we move forward, the challenge for policymakers and healthcare providers will be to decouple the cost of care from the quality of outcomes. Ensuring that treatment is affordable and accessible is the only way to lower the number of people who find themselves in need of inpatient crisis management. Until then, the high costs of inpatient care will remain a stark reminder of the work that remains to be done in achieving true parity for mental and substance use health in the United States.
For more information on the methodology and full scope of this analysis, please refer to the Peterson-KFF Health System Tracker, an essential resource for those tracking the evolving landscape of the U.S. health system.