Breast cancer is not a monolithic disease but a complex spectrum of biological subtypes, each defined by the molecular drivers that propel its growth. Among these, Hormone Receptor-positive (HR-positive) breast cancer stands as the most prevalent, accounting for approximately 70% of all diagnoses in women. While the sheer volume of cases makes it a focal point of global oncology, the narrative surrounding HR-positive breast cancer has shifted dramatically in recent years. What was once a diagnosis met with broad-spectrum treatments is now a field defined by precision medicine, long-term management strategies, and a burgeoning toolkit of targeted therapies.
As research continues to peel back the layers of tumor biology, the medical community is finding more reasons for optimism. Through the efforts of organizations like the Breast Cancer Research Foundation (BCRF) and global clinical trials, the transition from "one-size-fits-all" chemotherapy to highly specific endocrine and molecular interventions has redefined survival expectations for millions.
Main Facts: Defining the HR-Positive Subtype
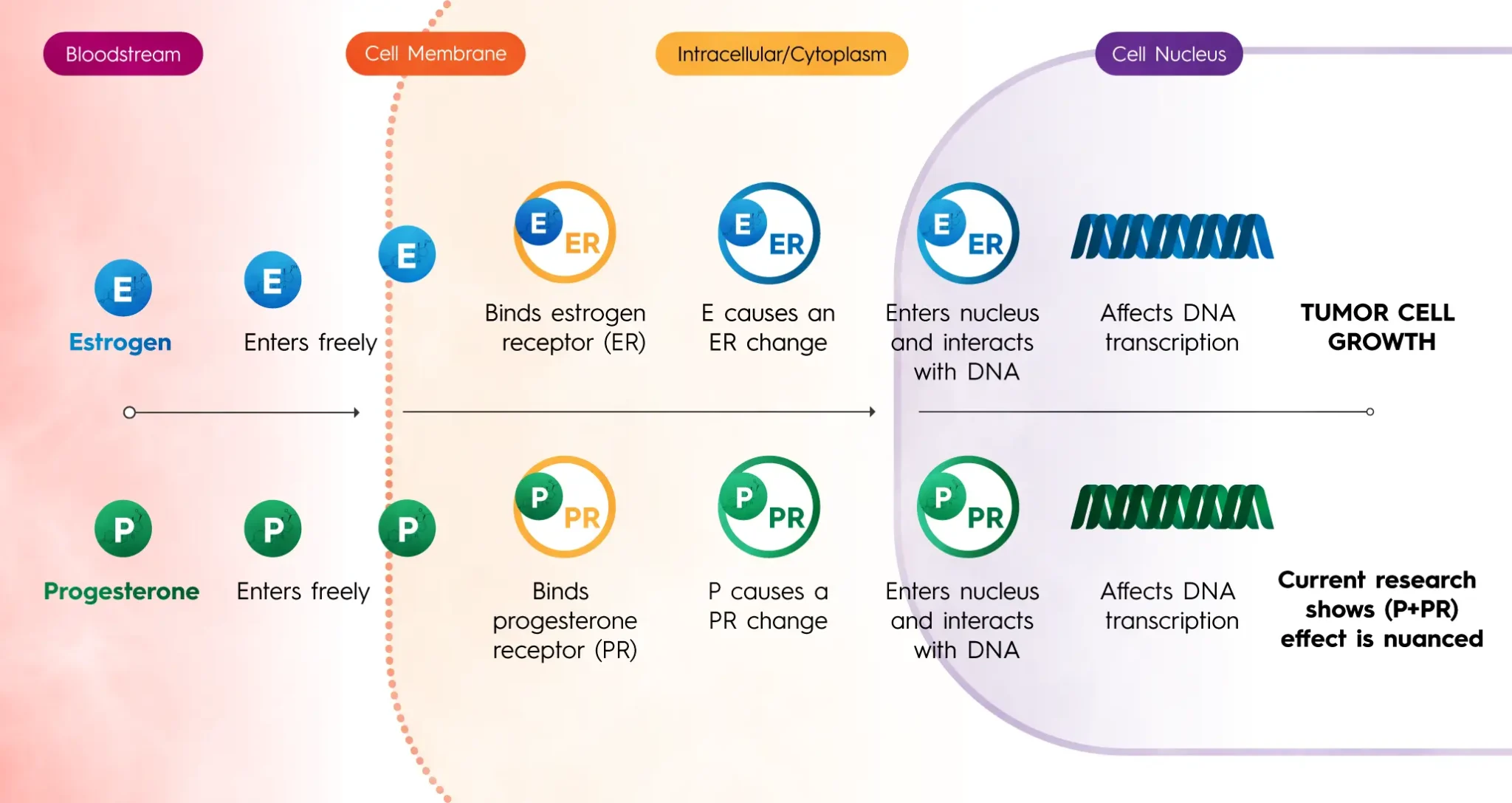
At its core, HR-positive breast cancer is defined by the presence of specific proteins—receptors—on the surface or inside the cancer cells. These receptors are designed to catch and bind to the hormones estrogen, progesterone, or both. In a healthy body, these hormones regulate various physiological functions; however, in HR-positive cancer, they act as high-octane fuel. When a hormone attaches to its corresponding receptor, it sends a biochemical signal to the cell nucleus, commanding the cancer to grow, divide, and spread.
The Receptor Profiles
Clinicians classify these tumors based on which receptors are present:
- ER-positive (ER+): The cells have receptors for estrogen.
- PR-positive (PR+): The cells have receptors for progesterone.
- HR-positive: Most patients are "double positive" (ER+/PR+), though some may be positive for only one.
This hormonal dependency is the "Achilles’ heel" of the subtype. Because the cancer relies on the body’s natural endocrine system to survive, it creates a clear target for therapy. This distinguishes HR-positive cancer from "Triple-Negative" breast cancer (which lacks estrogen, progesterone, and HER2 receptors) or HER2-positive cancer, which is driven by a specific protein overproduction.
Prevalence and Risk Factors
HR-positive breast cancer is the most common subtype across almost all demographics, but it is most frequently diagnosed in postmenopausal women. Age remains the most significant risk factor; as women age, the cumulative exposure to estrogen increases the statistical likelihood that a tumor will develop hormone sensitivity. While significantly rarer, HR-positive breast cancer also occurs in men, where the hormonal drivers are similar, though the clinical path to diagnosis often differs.
Chronology: A Half-Century of Therapeutic Evolution
The history of HR-positive breast cancer treatment is a testament to the power of iterative science. The journey from rudimentary surgery to oral precision medicine spans several decades of breakthrough discoveries.
The Early Era: Identifying the Driver (1960s–1970s)
In the mid-20th century, researchers first identified the correlation between estrogen and tumor growth. This led to the development of Tamoxifen, a Selective Estrogen Receptor Modulator (SERM). Approved in the 1970s, Tamoxifen revolutionized care by sitting in the estrogen receptor "lock," preventing the hormone "key" from entering. For the first time, doctors had a systemic way to starve the cancer without relying solely on cytotoxic chemotherapy.
The Rise of Aromatase Inhibitors (1990s–2000s)
While Tamoxifen blocked the receptors, scientists sought a way to stop the body from producing estrogen altogether. This led to Aromatase Inhibitors (AIs) like letrozole, anastrozole, and exemestane. By blocking the enzyme aromatase—which converts other hormones into estrogen in fat tissue—AIs became the gold standard for postmenopausal women, significantly reducing recurrence rates compared to Tamoxifen alone.
The Targeted Revolution (2015–Present)
The last decade has seen an explosion in "targeted therapies." In 2015, the approval of the first CDK4/6 inhibitor (palbociclib) marked a paradigm shift. These drugs do not target hormones directly; instead, they block the proteins responsible for cell division. When combined with endocrine therapy, they have doubled progression-free survival for many patients with advanced disease.
The 2023 Breakthrough: Oral SERDs
For over twenty years, Fulvestrant was the only Selective Estrogen Receptor Degrader (SERD) available, and it required painful monthly injections. In 2023, the FDA approved Elacestrant, the first oral SERD, followed by others like imlunestrant. These drugs don’t just block the receptor; they cause the receptor to break down and disappear, providing a vital new line of defense for patients whose cancers have become resistant to traditional therapies.
Supporting Data: Survival Metrics and the Reality of Late Recurrence
The data surrounding HR-positive breast cancer reflects both its treatability and its unique challenges. Currently, the five-year relative survival rate for localized HR-positive breast cancer is over 99%. However, the data also reveals a nuance specific to this subtype: the risk of late recurrence.
The "Marathon" of Treatment
Unlike other more aggressive subtypes that tend to recur within the first three to five years if they return at all, HR-positive tumors can remain dormant for a decade or more. Data suggests that the risk of recurrence remains steady for at least 20 years after the initial diagnosis.
- Clinical Response: This has led to the recommendation of extended endocrine therapy. While the standard was once five years, many patients are now advised to stay on medication for 10 years.
- Genomic Insights: Tools like Oncotype DX and MammaPrint now allow oncologists to analyze the activity of 21 to 70 different genes within a tumor. This data provides a "recurrence score," which tells doctors whether a patient actually needs chemotherapy or if they can safely be treated with hormone therapy alone. This has spared thousands of women from the toxicity of unnecessary chemo.
The Impact of CDK4/6 Inhibitors
In the metastatic setting, the addition of CDK4/6 inhibitors (ribociclib, abemaciclib) has shown significant gains in overall survival. In various clinical trials, these combinations have extended life by years, turning what was once a terminal diagnosis into a manageable chronic condition for a growing number of patients.
Official Responses: Institutional Perspectives and Expert Consensus
The medical community’s response to HR-positive breast cancer is coordinated through rigorous clinical guidelines and the advocacy of research-funding bodies. Organizations such as the BCRF emphasize that the progress seen today is the direct result of "sustained investment in foundational science."
The BCRF Stance
Investigators funded by the BCRF have been instrumental in nearly every major drug approval in the HR-positive space. Their official position highlights that "knowledge is power," emphasizing that understanding the molecular sub-classification of a tumor is the single most important step in a patient’s journey. They advocate for continued research into "treatment resistance," the process by which cancer cells learn to bypass hormonal blocks.
Regulatory Milestones
The FDA’s rapid-fire approval of Antibody-Drug Conjugates (ADCs) like trastuzumab deruxtecan (Enhertu) and sacituzumab govitecan (Trodelvy) for certain HR-positive patients represents an official recognition of the "HER2-low" category. This allows patients who were previously classified strictly as HR-positive to benefit from "smart bomb" therapies that deliver chemotherapy directly to cancer cells while sparing healthy tissue.
Implications: The Future of Care and De-escalation
The implications of current research trends point toward a future of "de-escalation" and "chronic management." As we look forward, the management of HR-positive breast cancer is moving in several transformative directions.
Moving Away from Chemotherapy
The most significant implication for patients is the ability to avoid chemotherapy. By using genomic testing and highly effective oral targeted drugs, the "chemo-first" mentality is being replaced. This improves the quality of life, allowing patients to maintain employment, care for families, and avoid long-term side effects like neuropathy or permanent hair loss.
Managing Resistance
The primary hurdle remaining is endocrine resistance—when a tumor stops responding to hormone blockers. The development of next-generation SERDs and inhibitors that target the PI3K/AKT/mTOR pathways is specifically designed to "re-sensitize" the cancer to hormone therapy. This iterative approach ensures that when one drug stops working, there is another waiting in the wings.
Quality of Life as a Metric of Success
In the past, survival was the only metric that mattered. Today, with patients living decades after an HR-positive diagnosis, "survivorship" has become a medical sub-specialty. The focus has shifted to managing the side effects of long-term hormone suppression, such as bone density loss and menopausal symptoms, ensuring that the years added to a patient’s life are lived with dignity and comfort.
Conclusion
HR-positive breast cancer remains a formidable challenge due to its prevalence and its ability to recur years later. However, the trajectory of the last fifty years—from the first Tamoxifen tablet to the latest oral SERDs and ADCs—demonstrates a field in constant, successful motion. For the 70% of women facing this diagnosis, the message from the scientific community is clear: the toolkit is larger than it has ever been, the treatments are smarter, and the hope for a long, healthy life is backed by robust, evolving science. Through continued research and clinical vigilance, the goal of transforming HR-positive breast cancer from a life-threatening event into a manageable condition is becoming a reality for patients worldwide.