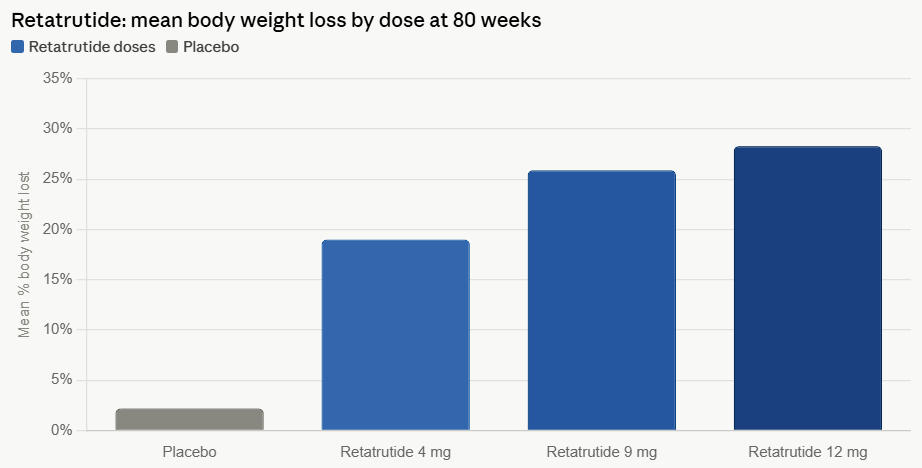
In the rapidly evolving landscape of metabolic medicine, Eli Lilly has positioned itself at the vanguard with its latest clinical breakthrough: retatrutide. As a triple hormone receptor agonist, this investigational drug has achieved what was once considered the exclusive domain of surgical intervention—delivering a staggering 28.3% average weight loss in Phase 3 trials. However, this clinical milestone brings with it a complex narrative regarding patient tolerability, muscle preservation, and long-term skeletal health that is currently commanding the attention of endocrinologists and industry analysts alike.
The TRIUMPH-1 Milestone: Unprecedented Efficacy
The primary data emerging from the TRIUMPH-1 trial serves as a landmark moment in the treatment of obesity. Over a course of 80 weeks, participants receiving the highest dose of retatrutide experienced weight reduction that rivals the outcomes of bariatric surgery. By targeting three separate hormone receptors—GLP-1, GIP, and glucagon—retatrutide modulates hunger, metabolism, and energy expenditure with a potency that surpasses existing monotherapy and dual-agonist treatments.
While the headline figure of 28.3% weight loss highlights the drug’s potential to address the most severe cases of obesity, the trial also demonstrated a dose-dependent response. Even at a 4 mg dose, patients reached nearly 20% weight loss with minimal escalation. This flexibility suggests that retatrutide could eventually provide a tiered, patient-centric approach to weight management, allowing clinicians to titrate the medication based on the specific needs of the individual.
A Chronology of Discovery and Clinical Development
The journey of retatrutide from a laboratory concept to a Phase 3 heavyweight has been characterized by rapid acceleration.
- Early Phase Development: Initially identified as a "triple-G" agonist, the molecule was designed to maximize the synergistic effects of the incretin system.
- The Phase 2 Proof-of-Concept: Early studies hinted at the drug’s superior efficacy compared to semaglutide and tirzepatide, prompting the initiation of the expansive TRIUMPH clinical program.
- Phase 3 Triumphs: The TRIUMPH-1 trial results were released in mid-2026, marking the first time a non-surgical intervention crossed the 25% weight loss threshold in a broad, randomized trial setting.
- Current Status: As of mid-2026, the scientific community is awaiting comprehensive body composition data, which will shed light on the exact ratio of fat-to-lean-tissue loss, a critical factor for the drug’s future regulatory approval.
Analyzing the Safety Profile: The Trade-off
Despite the enthusiasm surrounding its efficacy, the clinical profile of retatrutide is not without friction. Data from the TRIUMPH-1 trial indicates a higher discontinuation rate—11.3% at the highest dose—compared to competitors like tirzepatide (6.1%) and semaglutide (8.0%).
The primary reasons for treatment cessation remain gastrointestinal in nature: severe nausea and vomiting. However, a more distinct and somewhat concerning phenomenon has emerged: dysesthesia. Approximately 12.5% of participants on the highest dose reported abnormal skin sensations, including burning, tingling, or "pins and needles." While researchers characterize these events as generally mild to moderate, their prevalence is notably higher than in other GLP-1 programs, such as orforglipron, which reported only 1.2% incidence.
The scientific consensus on the etiology of this side effect remains speculative. Experts hypothesize that because GLP-1 and glucagon receptors are expressed on peripheral and central nerves, the drug’s potent activation of these receptors may be triggering these sensory irregularities. Alternatively, some researchers point to the rapid metabolic shift—including the depletion of essential electrolytes and B vitamins—as a potential culprit for nerve irritation.
Lean Mass and the Skeletal Impact
One of the most pressing concerns in the current weight-loss revolution is the "muscle-to-fat" ratio of the weight lost. Clinical data across the class of GLP-1 agonists suggests that 20% to 35% of total weight reduction is comprised of lean tissue, including muscle.
For a patient losing 70.3 lbs (the average on the high-dose retatrutide arm), this could equate to an estimated 14 to 24.6 lbs of muscle loss. This is not merely an aesthetic concern; loss of muscle mass is a primary driver of bone density decline. As muscle mass decreases, the dynamic strain on the skeleton is reduced, triggering "disuse signaling" that accelerates bone resorption.
The medical community is increasingly focused on this intersection of weight loss and bone health. A 2025 review in Nature Bone Research highlighted that rapid weight loss is associated with a 1% to 3% decline in Bone Mineral Density (BMD) for every 10% of body weight lost. Recent data from the AAOS 2026 meeting further complicated the picture, indicating that GLP-1 users exhibit a higher risk of osteoporosis (4.1%) compared to matched controls (3.2%).
The GIP Hypothesis: A Potential Protective Mechanism
While muscle loss remains a hurdle, there is emerging evidence that the GIP component of retatrutide may offer a "cushion" for bone health. Unlike pure GLP-1 agonists, GIP receptors are found on both osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells).
Studies on tirzepatide—which also hits the GIP receptor—have shown that patients experience less BMD loss than would be expected given the magnitude of their weight loss. Mechanistic reviews suggest that GIP activation may counteract some of the catabolic signals sent to the skeleton during rapid caloric deficit. Scientists are now investigating whether retatrutide’s triple-agonist design provides a superior protective effect for bone material properties compared to dual or single agonists.
Official Perspectives and Market Implications
The industry response to these findings has been a mix of tempered optimism and cautious pragmatism.
Kenneth Custer, Executive Vice President of Lilly Cardiometabolic Health, emphasized the drug’s role in a broader portfolio, noting, "Together with Zepbound and Foundayo, retatrutide could build on Lilly’s commitment to match treatments to the needs and preferences of patients." Lilly’s strategy appears to be one of segmentation: offering a range of options where some drugs prioritize maximum potency (retatrutide), while others prioritize a "balanced" profile (tirzepatide).
Market analysts echo this sentiment. Trung Huynh of RBC Capital Markets dubbed the data a "clean win" for Lilly, citing the best-in-class efficacy. Conversely, analysts at William Blair have offered a more conservative outlook, suggesting that the tolerability profile of retatrutide might limit its primary use to the "higher end of the BMI spectrum," while tirzepatide will likely retain its status as the "go-to" medication for the broader population due to its superior tolerability.
Future Implications: The Next Generation
As the medical community prepares for the potential launch of retatrutide, the focus is shifting toward "next-generation" interventions. There is a burgeoning interest in peptides like SciWind Bio’s XW020, which are being specifically engineered to preserve muscle mass during weight loss.
Furthermore, the medical field is entering an era of "precision endocrinology," where the goal is not just weight loss, but "quality weight loss." This involves monitoring body composition, bone mineral density, and micronutrient levels as standard practice for patients on potent weight-loss therapies.
The arrival of retatrutide signifies that we have reached a threshold of efficacy that was previously unimaginable. However, the path forward requires a rigorous investigation into long-term safety, particularly regarding the long-term impact on the musculoskeletal system. As clinicians learn to manage the unique side-effect profile of this triple agonist, the drug is poised to become a vital, if complex, tool in the ongoing battle against the global obesity epidemic.
Whether retatrutide becomes the standard of care or a specialized treatment for the most extreme cases remains to be seen. What is clear is that the conversation has shifted from "can we lose the weight" to "how do we lose it safely and sustainably."