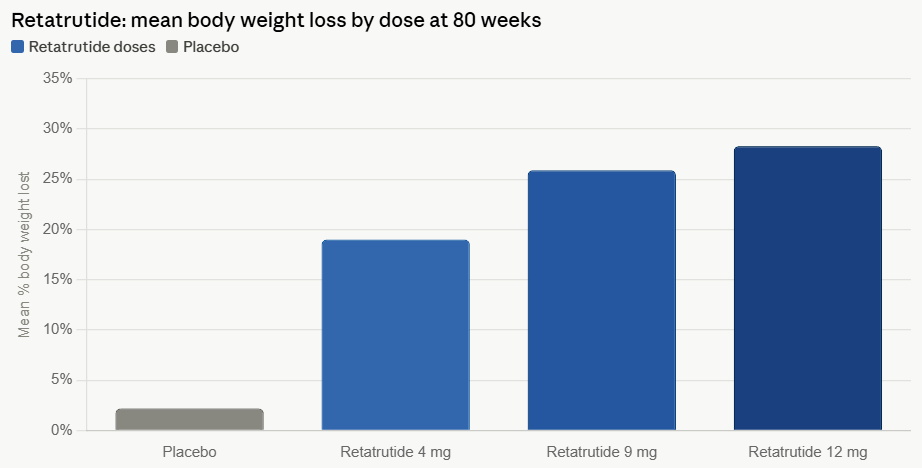
In the rapidly evolving landscape of metabolic medicine, Eli Lilly has reached a new milestone with its experimental triple-hormone receptor agonist, retatrutide. Recent Phase 3 clinical trial data from the TRIUMPH-1 study reveals that the drug can induce an average weight loss of 28.3% over 80 weeks at its highest dosage. While these figures represent a performance tier once reserved for bariatric surgery, they have simultaneously ignited a complex debate regarding the trade-offs between potent efficacy and the physiological toll of rapid weight reduction.
As the medical community scrutinizes these results, the pharmaceutical sector is grappling with a central question: Is the quest for "best-in-class" weight loss causing us to overlook significant side effects, including muscle atrophy and neurological disruptions?
The Clinical Landscape: Efficacy vs. Tolerability
The TRIUMPH-1 trial results present a compelling, if cautionary, case for the next generation of anti-obesity medications (AOMs). Retatrutide functions as a triple agonist, targeting the receptors for glucagon, glucose-dependent insulinotropic polypeptide (GIP), and glucagon-like peptide-1 (GLP-1). By hitting these three biological targets simultaneously, the drug creates a powerful synergy that suppresses appetite and modulates metabolic rate more aggressively than current GLP-1 mono-agonists or dual-agonists.
However, the efficacy of the 12 mg dose comes at a price. Clinical data indicates that 11.3% of participants discontinued the trial specifically due to adverse events. To put this in perspective, this discontinuation rate exceeds that of existing therapies, such as tirzepatide (6.1%), semaglutide (8.0%), and orforglipron (10.3%). This trend suggests that while retatrutide may represent the pinnacle of weight-loss potential, its tolerability profile may limit its application to a specific subset of patients who can endure more intense gastrointestinal and systemic side effects.
A Chronological Progression of GLP-1 Development
The journey toward retatrutide did not occur in a vacuum; it is the latest chapter in a multi-decade effort to address the global obesity epidemic.
- The Early Years (2010–2020): The initial success of GLP-1 receptor agonists (like liraglutide) for Type 2 diabetes shifted the paradigm toward weight management. Researchers discovered that higher doses of these agents, originally designed for glucose control, significantly influenced satiety signals in the brain.
- The Rise of Dual Agonism (2021–2024): With the introduction of tirzepatide, which combines GIP and GLP-1 receptor agonism, weight loss outcomes jumped into the 20% range. This established a new standard of care, proving that dual-pathway activation was superior to single-pathway stimulation.
- The Triple Agonist Era (2025–Present): With the development of retatrutide, Eli Lilly sought to incorporate glucagon receptor activation, which is believed to increase energy expenditure. The TRIUMPH-1 trial confirmed that this triple-pronged approach could push weight loss toward the 30% mark, effectively challenging the necessity of invasive surgical interventions for many patients.
Supporting Data: Dissecting the Side Effect Profile
The most concerning findings from the recent trials involve "dysesthesia"—a neurological sensation characterized by burning, tingling, or a "pins and needles" feeling. Approximately 12.5% of patients on the highest dose of retatrutide reported these sensations.
While researchers are still investigating the exact etiology of dysesthesia, several hypotheses have emerged. The first is that the high-intensity activation of GLP-1 and glucagon receptors—which are present on both central and peripheral nerves—may interfere with normal signaling. The second, perhaps more clinically actionable, hypothesis points to the rapid depletion of essential nutrients, particularly B vitamins and electrolytes, resulting from drastically reduced caloric intake and rapid fat loss.
Furthermore, the data regarding body composition is particularly sobering. Historically, weight loss induced by GLP-1 therapies is not comprised entirely of adipose tissue. In fact, lean tissue—which includes vital muscle mass—accounts for 20% to 35% of the total weight lost. In the case of retatrutide, with an average loss of 70.3 pounds, clinical projections suggest that patients could be losing between 14 and 24.6 pounds of muscle.
Official Responses and Strategic Positioning
Eli Lilly’s leadership remains optimistic about the role of retatrutide within its broader portfolio. Kenneth Custer, executive vice president and president of Lilly Cardiometabolic Health, stated, "TRIUMPH-1 highlights the importance of options and the potential for retatrutide to help people across various stages of their obesity journey."
Lilly’s strategy appears to be one of "segmentation." By offering a tiered range of medications—including Zepbound, the upcoming Foundayo, and eventually retatrutide—the company aims to match the intensity of the treatment to the severity of the patient’s condition. Analysts, such as Trung Huynh of RBC Capital Markets, have praised the drug’s "best-in-class efficacy," viewing it as a major win for the company’s competitive positioning against rivals like Novo Nordisk.
However, dissenting voices from firms like William Blair highlight a more pragmatic outlook. They suggest that because of the adverse event profile, tirzepatide will likely remain the "gold standard" or "go-to" medication for the general population, with retatrutide reserved for those at the higher end of the Body Mass Index (BMI) spectrum who require more drastic, rapid intervention.
The Bone Density and Muscle Preservation Crisis
Perhaps the most significant long-term concern for the next generation of weight loss drugs is the preservation of skeletal integrity and muscle mass. As weight loss reaches these unprecedented levels, the body undergoes a rapid reduction in the physical load placed upon the skeleton.
According to research published in Nature Bone Research in 2025, rapid weight loss is associated with a 1% to 3% decline in bone mineral density (BMD) for every 10% of body weight lost. The mechanism is a feedback loop: reduced physical stress leads to increased bone resorption and decreased bone formation. Five-year follow-up data from the 2026 AAOS meeting corroborated this, showing that long-term GLP-1 users faced a statistically higher risk of osteoporosis (4.1%) compared to matched controls (3.2%).
However, there is a glimmer of hope in the biological pathways being explored. Emerging studies indicate that GIP receptor activation may have a protective effect on bone tissue. Researchers believe that because GIP receptors are found on osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells), the GIP-agonism present in drugs like tirzepatide might partially mitigate the bone loss usually seen with rapid weight reduction. This "protective" nuance is currently a major focus for pharmaceutical R&D, as companies race to develop "muscle-sparing" weight loss agents like SciWind Bio’s XW020.
Future Implications: The Road Ahead
The success of retatrutide is a testament to the power of human ingenuity in metabolic science. It has proven that we can, with enough pharmacological precision, manipulate the human body to reverse obesity at rates previously considered impossible. Yet, the data serves as a stark reminder that medicine is rarely without consequence.
As we look toward the future, the pharmaceutical industry must pivot its focus from pure weight-loss efficacy to "weight-quality" efficacy. The goal of 2027 and beyond will not simply be to help patients reach a target weight, but to do so while preserving their muscle mass, protecting their bone density, and avoiding neurological side effects like dysesthesia.
For the patient, the implications are clear: the landscape of obesity treatment is becoming increasingly personalized. While the "magic bullet" of 28.3% weight loss is now a reality, the decision to pursue such a path will require a careful, nuanced assessment of the risks versus the benefits—a conversation that will likely define the next decade of endocrinology. As the scientific community continues to publish follow-up data from the TRIUMPH-1 trial, the industry will be watching closely to see if retatrutide can be optimized to balance its extraordinary power with the long-term safety profiles that patients and clinicians demand.