By [Your Name/Journalistic Desk]
Updated: May 15, 2026
The federal government is fundamentally reshaping its approach to Medicaid oversight, moving away from historical patterns of collaborative auditing toward a more aggressive, punitive posture. At the heart of this shift is the "Comprehensive Regulations to Uncover Suspicious Healthcare" (CRUSH) initiative, a strategy spearheaded by the Centers for Medicare and Medicaid Services (CMS) that prioritizes the withholding of federal funds over traditional investigative cooperation.
As states grapple with the fiscal volatility of the 2025 reconciliation law, this new enforcement strategy—specifically the increased reliance on deferrals and withholds—has introduced a level of uncertainty that threatens the stability of Medicaid programs nationwide.
Main Facts: The Architecture of the CRUSH Initiative
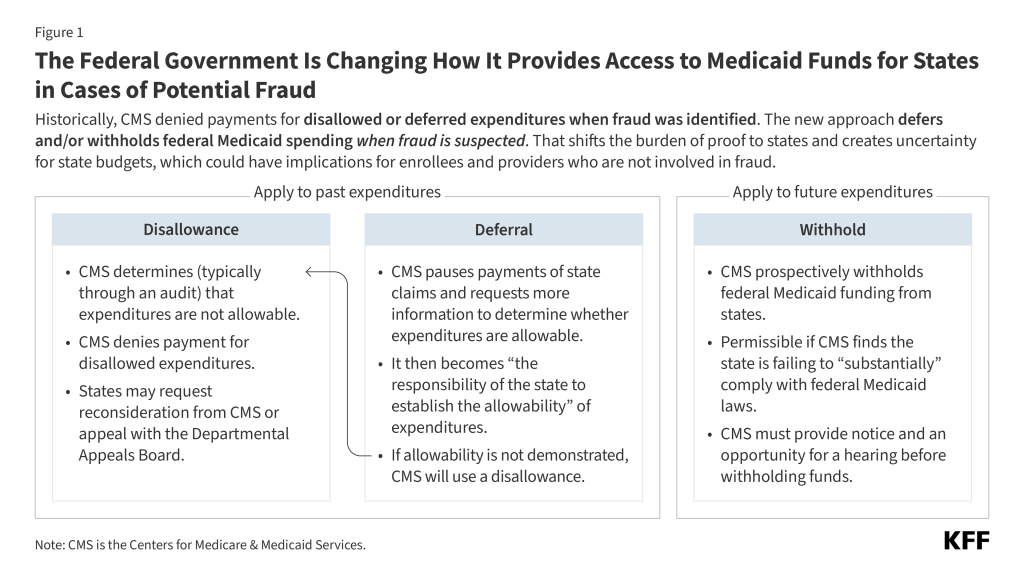
Historically, the relationship between CMS and state Medicaid agencies was defined by a shared interest in program integrity. When fraud, waste, or abuse was identified, federal and state partners typically engaged in audits followed by reconciliation. If a portion of spending was deemed unallowable, CMS would issue a "disallowance," effectively denying the federal share of those specific costs.
The CRUSH initiative departs from this by shifting the burden of proof onto the states before fraud is even fully substantiated. By employing "deferrals" (pausing payments while documentation is gathered) and "withholds" (halting funds pending legal or administrative outcomes), CMS is effectively utilizing federal funding as a lever of compliance.
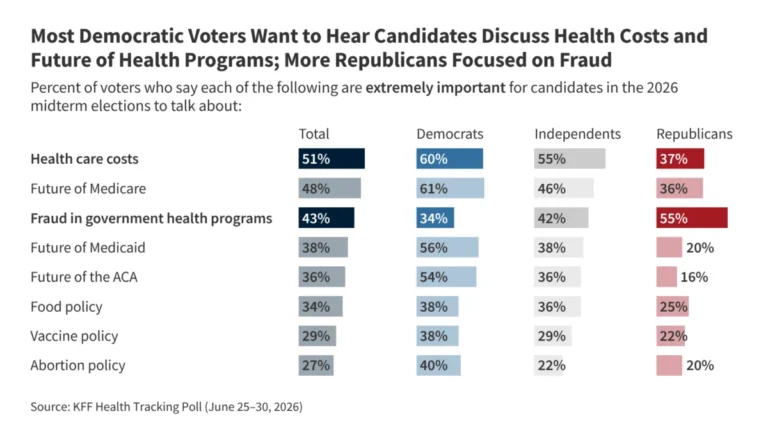
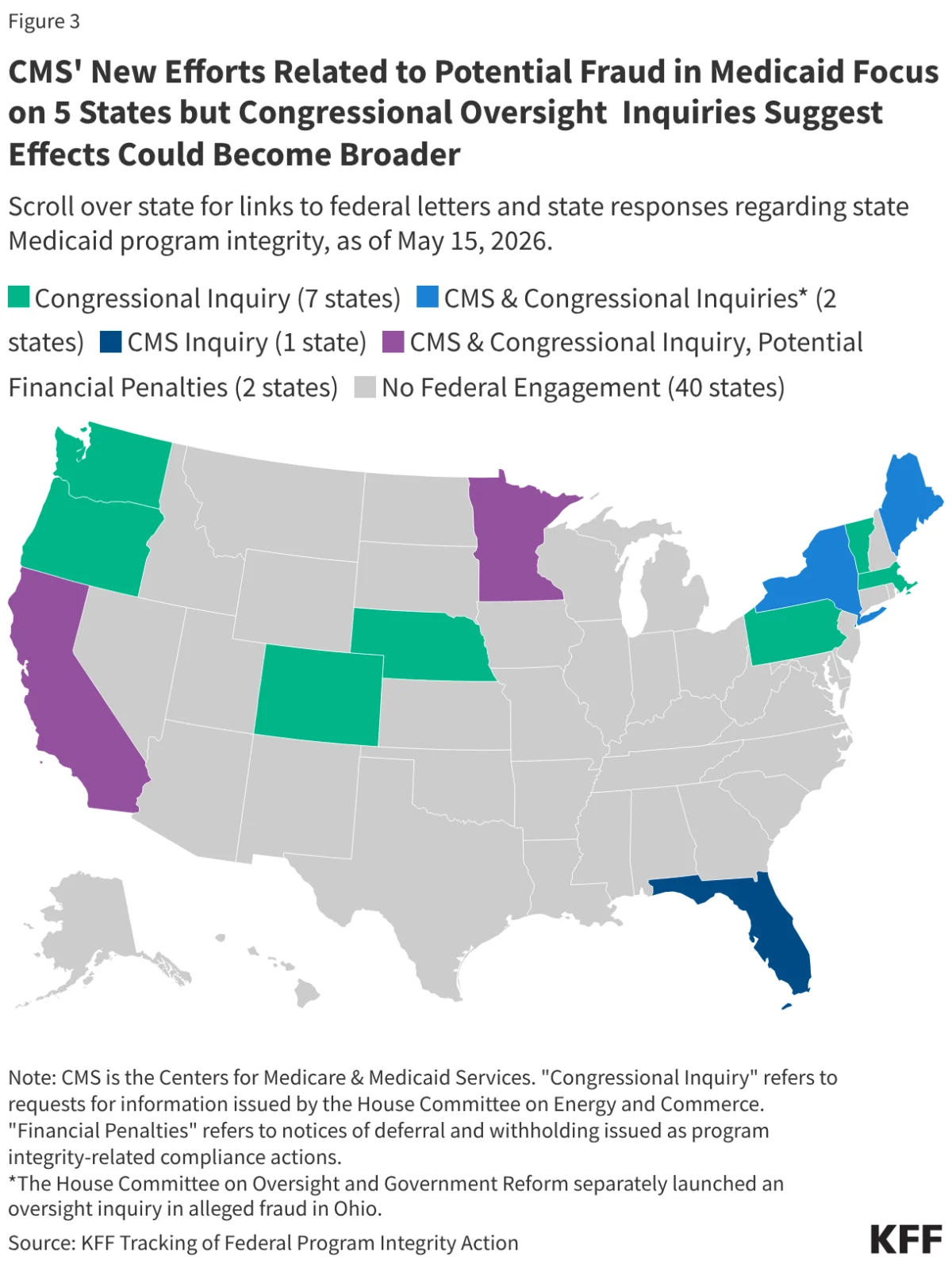
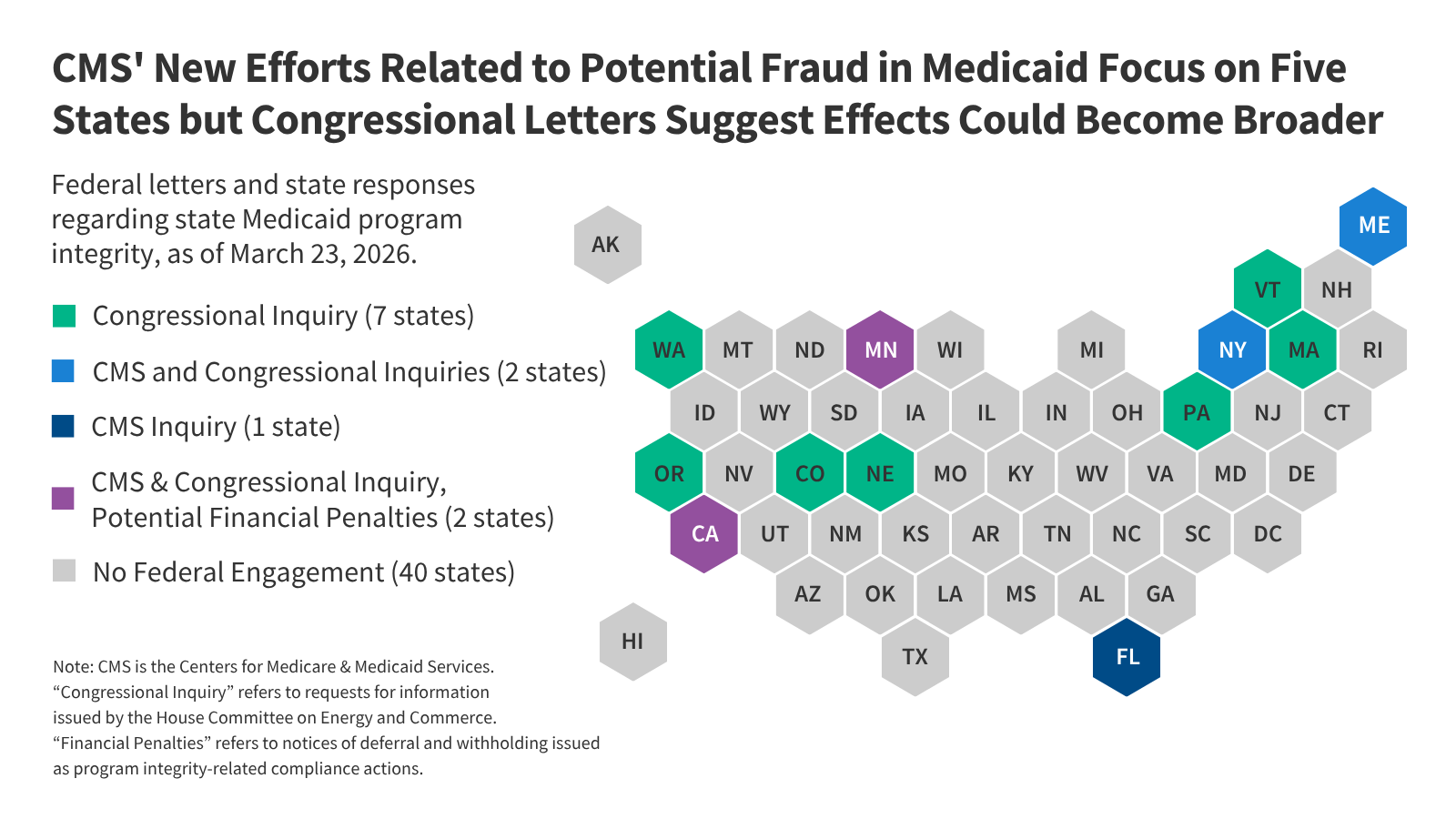
The initiative is not merely administrative; it is political. Current data indicates a distinct focus on states with Democratic governors, including Minnesota, California, Maine, and New York. This geographical concentration has prompted significant concern among policy experts who argue that the scale of these financial maneuvers—most notably the $515 million proposed withholding in Minnesota—exceeds any historical precedent for addressing compliance issues.
Chronology: A Timeline of Escalation
The recent escalation in federal oversight can be mapped through a series of key actions taken between late 2025 and early 2026:
- Late 2025: CMS signals a shift in enforcement priorities, moving away from reactive auditing toward preemptive fund sequestration.
- January 13, 2026: Minnesota formally requests an administrative hearing to challenge a proposed $515 million withholding of federal Medicaid funds.
- January 14, 2026: CMS officially notifies Minnesota of the withholding, citing non-compliance concerns related to potential future fraud.
- January 30, 2026: Minnesota submits a revised corrective action plan in an attempt to stave off the loss of federal support.
- March 20, 2026: CMS formally accepts Minnesota’s corrective action plan, momentarily pausing the immediate threat of withholding, though the regulatory environment remains tense.
- March 25, 2026: Reports confirm that four additional states have received formal requests for information regarding program integrity, while the House Committee on Energy and Commerce expands its investigation to 11 states total.
Supporting Data: Understanding Financial Mechanisms
To understand why the CRUSH initiative is causing such alarm, one must distinguish between the three primary tools in the federal arsenal:
1. Disallowances: The Historical Standard
A disallowance occurs after the fact. CMS identifies specific expenditures that do not comply with federal regulations and denies the federal matching funds. While legal appeals through the Departmental Appeals Board can take upwards of 15 years to resolve, they have historically been reserved for well-documented cases of overpayment or fraud.
2. Deferrals: The New Pressure Point
Deferrals are temporary pauses in funding used while an investigation is underway. Under CRUSH, the frequency of these deferrals has spiked. Because a deferral results in an immediate loss of federal cash flow, it forces states to operate with an unexpected budget hole, often before they have the opportunity to prove the expenditures were legitimate.
3. Withholds: The "Nuclear" Option
Withholds are intended for states that are fundamentally failing to comply with Medicaid law. Historically, these were capped at 1% to 10% of specific administrative costs. The current effort to withhold nearly 20% of Minnesota’s annual federal Medicaid share represents an unprecedented deviation from this standard, treating suspected future fraud with the same severity as institutional non-compliance.
Official Responses and Political Landscape
The federal government maintains that these measures are essential to protecting taxpayer dollars. A press release from the current administration highlights that the crackdown is necessary to ensure "affordability and accountability." They argue that states must be more proactive in preventing fraud, and that federal funds should not be distributed until states can definitively prove that the underlying healthcare services are not tainted by abuse.
Conversely, state leaders and groups like the National Association of Medicaid Directors (NAMD) have warned against the "weaponization" of these financial tools. The NAMD has suggested that rather than withholding funds—which hurts the most vulnerable enrollees—CMS should focus on:
- Standardizing data-sharing protocols to detect fraud early.
- Providing technical assistance for states to improve internal auditing.
- Allowing for "good faith" periods when states are actively implementing corrective action plans.
The House Committee on Energy and Commerce, meanwhile, has taken a dual-track approach, using its oversight power to demand internal documentation from 11 states, further increasing the administrative burden on state agencies that are already struggling to implement the 2025 reconciliation law.
Implications: The Human and Fiscal Cost
The ripple effects of the CRUSH initiative extend far beyond state treasuries. The consequences are likely to be felt by the most vulnerable populations:
Fiscal Instability for States
Because states must balance their budgets, a surprise deferral or withholding creates a "fiscal cliff." When federal funding is yanked, states may be forced to choose between borrowing money, draining rainy-day funds, or cutting services. The uncertainty itself creates a "chilling effect," where states may shy away from expanding services or programs for fear of triggering a federal audit.
The Impact on Providers and Enrollees
The most significant fear among health advocates is the impact on non-fraudulent providers and patients. If a state faces a massive budget shortfall, the most common levers for cost-cutting include:
- Reduced Provider Rates: Lowering reimbursement rates often leads to physician shortages, as doctors refuse to accept Medicaid patients due to inadequate pay.
- Benefit Trimming: States may be forced to drop optional services—such as dental, vision, or mental health therapy—to save money.
- Administrative Burdens: Providers already operating under thin margins are now being subjected to increased, redundant audits, leading to burnout and, in some cases, the closure of smaller clinics that cannot afford the administrative cost of compliance.
Long-term Policy Consequences
The combination of the 2025 reconciliation law—which already mandated deep cuts and introduced new, complex work requirements—and the CRUSH initiative creates a "perfect storm" for state Medicaid programs. As states attempt to navigate the new work requirements, they are now being hit with increased oversight that mandates even more paperwork.
Ultimately, this new era of Medicaid oversight suggests that the federal government is prioritizing the mitigation of potential fraud over the continuity of patient care. Whether this strategy will actually result in a more efficient program or merely a more fragmented one remains the central question of the 2026 legislative year. As more states receive letters from CMS and the House committee, the national discourse around the balance between federal oversight and state autonomy is likely to intensify, potentially leading to legal challenges that could redefine the Medicaid program for the next decade.