The landscape of multiple myeloma treatment has shifted from a paradigm of chronic disease management to one of durable, high-depth responses. At the epicenter of this clinical revolution lies the B-cell maturation antigen (BCMA)—a protein expressed ubiquitously on the surface of malignant plasma cells. As the pharmaceutical industry and clinical researchers push the boundaries of immunotherapy, BCMA-targeted agents, including Chimeric Antigen Receptor (CAR) T-cell therapies and bispecific antibodies, have become the gold standard for refractory patients. However, this clinical success has birthed a new frontier of complex challenges.
Main Facts: The Rise of BCMA-Targeted Therapy
Multiple myeloma, characterized by the clonal proliferation of plasma cells in the bone marrow, has historically been marked by inevitable relapse. The introduction of BCMA-targeted therapies has altered this trajectory. BCMA is an ideal target because of its limited expression on non-malignant tissues, making it a "sweet spot" for immunotherapy.
Current therapeutic approaches utilize two primary modalities:
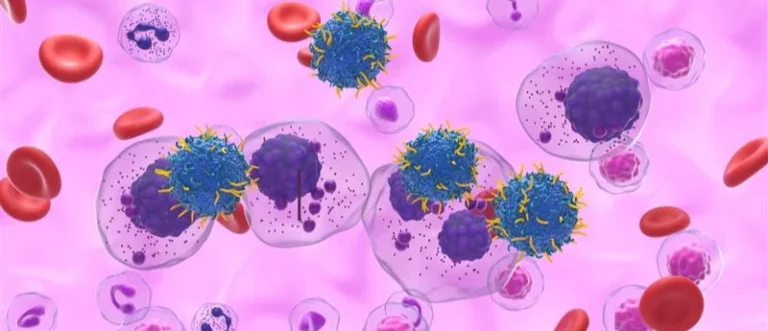
- CAR T-cell therapies: Genetically engineering a patient’s own T-cells to recognize and eliminate BCMA-expressing myeloma cells.
- Bispecific T-cell Engagers (BiTEs): Off-the-shelf molecules that bridge malignant cells and T-cells to trigger an immune-mediated kill.
While these therapies have achieved unprecedented complete response (CR) rates in heavily pre-treated populations, they have introduced a novel spectrum of toxicities, most notably Immune Effector Cell-Associated Hematotoxicity (ICAHT). As the field moves toward ASCO 2026, the primary focus is no longer just on achieving remission, but on durability and the management of long-term side effects.
Chronology: The Evolution of Targeted Myeloma Care
The journey toward BCMA-targeted therapy did not occur in a vacuum. It is the culmination of decades of research into plasma cell biology.
- 2010–2015: The "Target Identification" phase. Researchers validate BCMA as a high-density target on myeloma cells, setting the stage for monoclonal antibodies and antibody-drug conjugates (ADCs).
- 2017–2020: The "CAR T-cell Emergence." Initial clinical trials show rapid, deep responses in patients who had failed proteasome inhibitors and immunomodulatory drugs (IMiDs).
- 2021–2023: Regulatory Approval and Real-World Evidence. The FDA grants approvals for the first wave of BCMA CAR T-cell therapies, followed closely by the introduction of bispecific antibodies (e.g., teclistamab, elranatamab).
- 2024–2025: The "Relapse and Resistance" phase. Clinicians begin to see the limits of single-target BCMA therapies, noting antigen escape and the exhaustion of T-cell pools.
- 2026 (The Current Horizon): The focus shifts toward "Sequencing and Management." As presented in the latest ASCO 2026 summaries, the clinical conversation is now centered on managing the toxicities of sequential BCMA therapies and navigating the post-CAR T-cell landscape.
Supporting Data: Understanding the Clinical Efficacy and Toxicity
Clinical data from the past 24 months underscores the efficacy of BCMA-targeted therapy, but it also highlights the precarious nature of these treatments.
Efficacy Metrics
In pivotal trials, BCMA CAR T-cell therapies have demonstrated overall response rates (ORR) exceeding 80% in patients who have failed at least three prior lines of therapy. For many, these therapies represent the final bridge to long-term disease control. However, data indicates that the "tail of the curve" is shrinking due to subsequent relapses, necessitating a strategy for post-BCMA intervention.
The Challenge of Hematotoxicity
One of the most pressing data points in current hematology literature is the incidence of prolonged Immune Effector Cell-Associated Hematotoxicity (ICAHT). Unlike the transient cytopenias seen with traditional chemotherapy, ICAHT can persist for months after the initial infusion.
- Neutropenia: Reported in approximately 30-40% of patients post-CAR T.
- Thrombocytopenia: Frequently observed, often requiring prophylactic support and careful monitoring.
- Infection Risk: The interplay between BCMA-targeted therapy and hypogammaglobulinemia creates a significant risk of opportunistic infections, which remain a leading cause of non-relapse mortality.
Official Responses and Expert Consensus
Leading clinical societies, including the American Society of Clinical Oncology (ASCO), have emphasized that the integration of these agents requires a multidisciplinary approach.
According to the latest consensus reports, hematologists are being urged to move away from "trial-and-error" prescribing. Instead, the focus is on the strategic integration of immunomodulatory agents. The expert consensus for 2026 emphasizes:
- Early Intervention: Addressing cytokine release syndrome (CRS) and neurotoxicity (ICANS) with standardized protocols to prevent progression to severe grades.
- Longitudinal Monitoring: Utilizing bone marrow biopsies and blood counts to monitor for residual disease, while simultaneously managing the long-term hematologic impacts of treatment.
- Cross-Platform Sequencing: Understanding how to effectively transition a patient from an ADC (like belantamab mafodotin) to a CAR T-cell therapy or a bispecific antibody without inducing additive toxicity.
Implications for Clinical Practice
The implications of this shift are profound. For the average community hematologist, the complexity of managing a BCMA-treated patient is akin to managing a transplant patient.
Expanding Relapse Options
The most critical implication is the need for a post-CAR T-cell strategy. Researchers are now exploring:
- Dual-targeting: Investigating GPRC5D or CD19 in combination with BCMA to bypass antigen escape.
- T-cell fitness: Studies are exploring how to improve the quality of the apheresis product, even in patients who have been exposed to multiple lines of toxic chemotherapy.
- Maintenance therapies: The use of low-dose IMiDs or proteasome inhibitors following immunotherapy to "keep the pressure on" the malignant clone.
Bridging the Knowledge Gap
The move toward specialized care means that educational resources are no longer optional—they are a prerequisite for patient safety. With the release of clinical guides on managing prolonged hematotoxicity, practitioners are finally receiving the standardized framework needed to manage patients in the clinic, rather than just within the confines of clinical trials.
Conclusion: The Path Forward
The "BCMA Era" of multiple myeloma has provided patients with years of life that were previously unimaginable. Yet, as we look toward the remainder of 2026 and beyond, it is clear that the technology alone is insufficient. Success depends on our ability to mitigate the physiological toll of these treatments and to innovate beyond the first line of immunotherapy.
For clinicians, the mandate is clear: keep pace with the rapidly evolving data on antigen escape and toxicity management. For patients, the evolution of these treatments offers the hope of chronic disease management in a condition that was once uniformly fatal. The path ahead is complex, but with the integration of new clinical insights and robust management strategies, the oncology community is better equipped than ever to navigate the frontiers of multiple myeloma.
Are you ready to optimize your practice?
The latest clinical insights, including the essential ASCO 2026 abstracts and comprehensive guides on managing immune effector cell-associated hematotoxicity, are available in our latest professional eBook. Download the guide to gain practical, actionable insights for your clinic today.
Registration is required to access the full report. Access is provided free of charge to healthcare professionals.