For decades, the KRAS gene—a master regulator of cellular signaling—was considered the "Holy Grail" of oncology, yet it remained frustratingly out of reach. Often described as "undruggable" due to its smooth, featureless surface, KRAS mutations drive a vast array of cancers, including some of the most aggressive forms of lung, colorectal, and pancreatic malignancies.
When the first generation of KRAS G12C inhibitors, such as sotorasib and adagrasib, finally broke through this barrier, they were celebrated as scientific triumphs. However, clinicians soon discovered that these molecules faced a fundamental biological hurdle: they were designed to lock the protein in an inactive state, but cancer cells are notoriously efficient at circumventing these traps, leading to rapid drug resistance.
Merck has taken a fundamentally different approach with its novel candidate, calderasib. Rather than seeking to create the most potent single-agent inhibitor, Merck’s researchers have prioritized "combinability." By designing a drug that is highly specific to the mutant protein while remaining compatible with other therapeutic modalities, Merck is positioning calderasib not just as a standalone treatment, but as the cornerstone of future combination regimens.
The Evolution of KRAS Inhibition: A Chronology
To understand the significance of calderasib, one must look at the trajectory of KRAS research.
The "Undruggable" Era (1980s–2010s)
KRAS was identified as a critical oncogene in the early 1980s. Because the protein is a molecular switch that toggles between "on" (GTP-bound) and "off" (GDP-bound) states to control cell division, mutations—specifically at the G12C position—keep the switch permanently locked in the "on" position, driving uncontrolled tumor growth. For thirty years, the lack of a suitable "pocket" on the protein surface for a small molecule to bind made drug development impossible.
The First Generation (2020–2023)
The paradigm shifted with the discovery of the "switch-II pocket," a small crevice that appears only when the protein is in its inactive state. First-generation inhibitors were designed to exploit this, effectively trapping the protein in the inactive form. However, because cancer cells keep most KRAS molecules in the active state, these drugs only addressed a fraction of the total target population. Consequently, tumors quickly developed compensatory resistance pathways.
The "Combinability" Pivot (2024–Present)
Recognizing the limitations of monotherapy, Merck pivoted to a strategy of synergistic inhibition. The development of calderasib represents a move away from the "magic bullet" philosophy toward a modular approach. By optimizing the molecule to be highly selective—thereby sparing wild-type KRAS and reducing systemic toxicity—Merck ensured that the drug could be safely paired with other agents, such as EGFR inhibitors (cetuximab) and standard chemotherapy.
Supporting Data: The KANDLELIT-001 Clinical Evidence
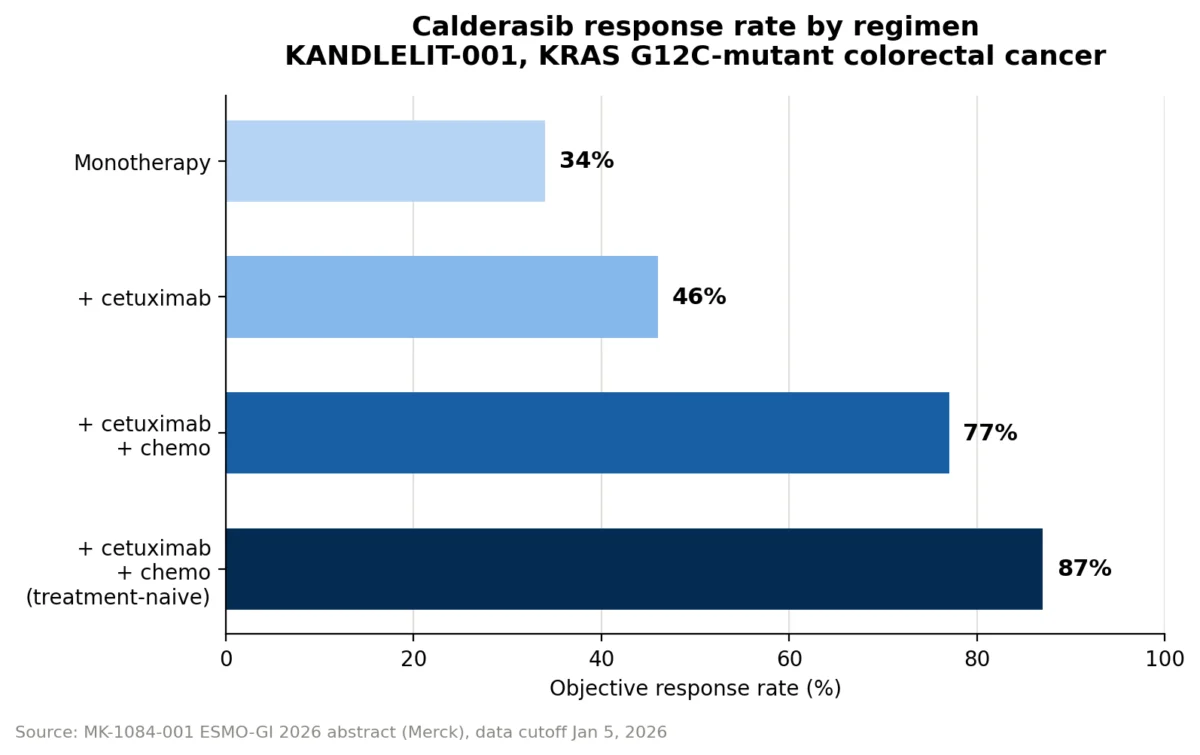
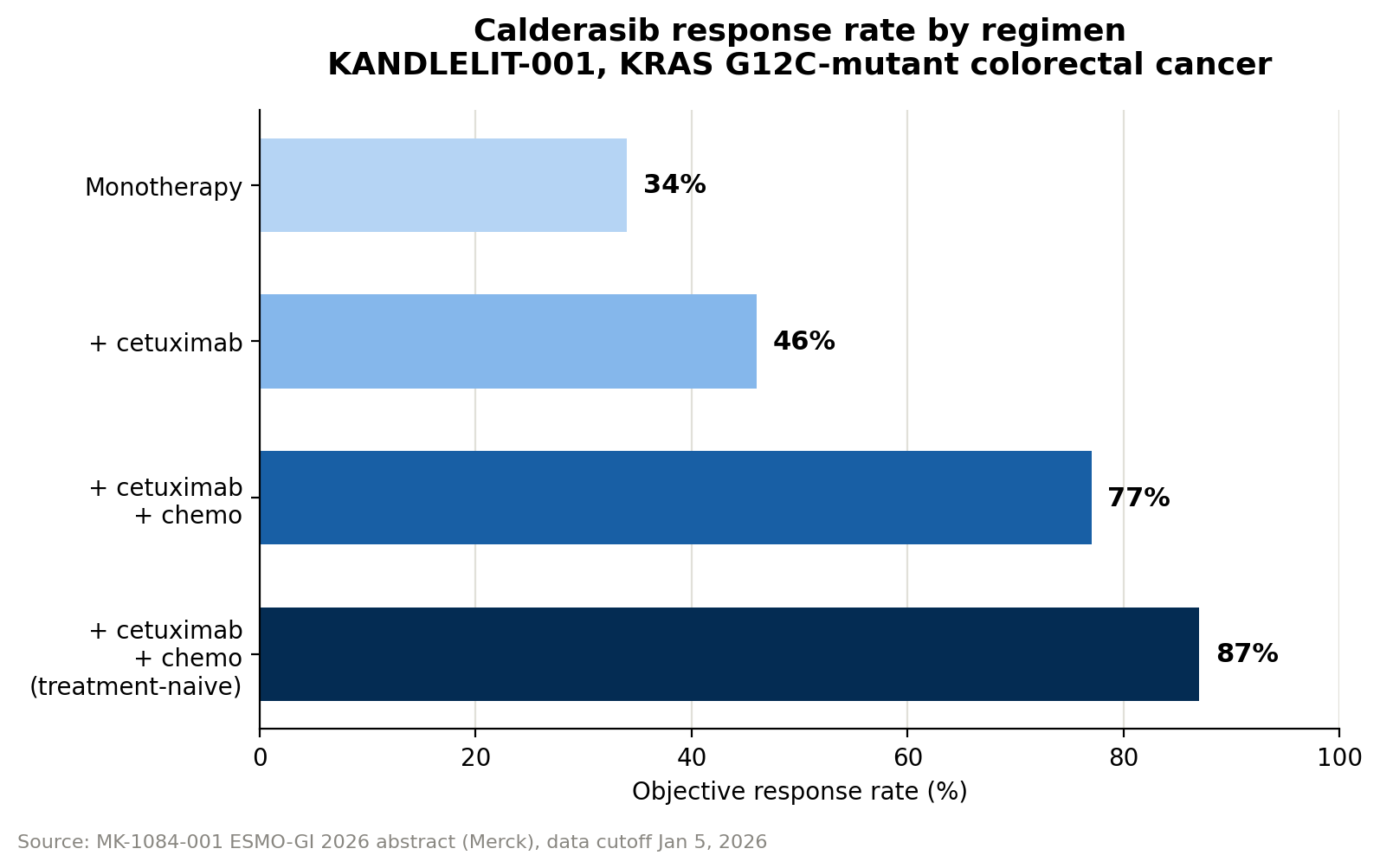
The KANDLELIT-001 Phase 1 trial serves as the primary proving ground for the calderasib thesis. The results suggest that while the drug shows moderate activity as a monotherapy, its true power lies in its ability to amplify the effects of other treatments.
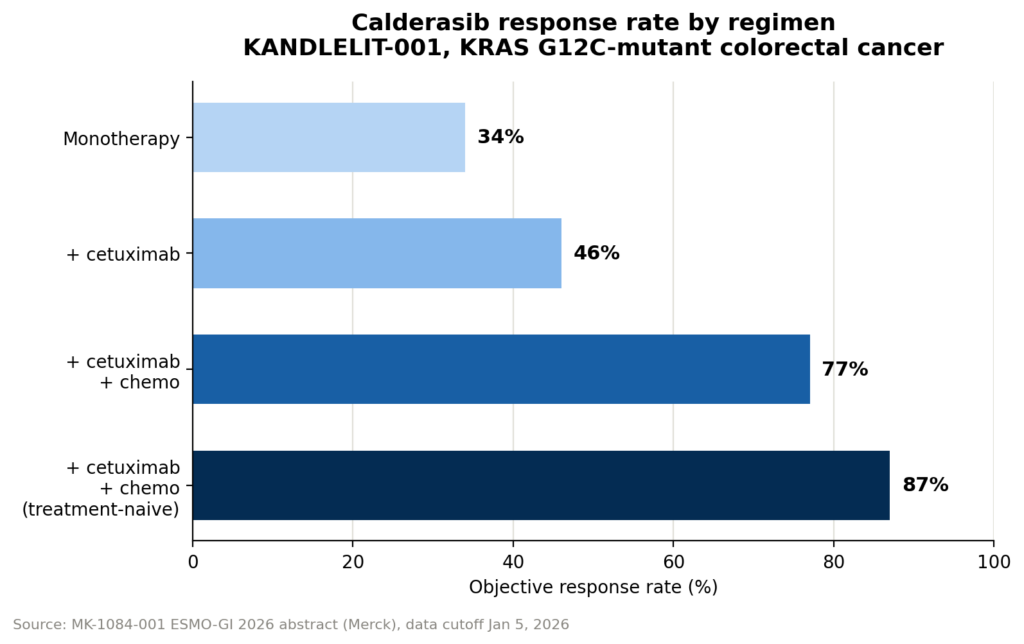
Objective Response Rates (ORR)
- Monotherapy: 34% ORR.
- Doublet (Calderasib + Cetuximab): 46% ORR.
- Triplet (Calderasib + Cetuximab + Chemotherapy): 77% ORR.
- Triplet (Treatment-Naïve Patients): 87% ORR.
These figures illustrate a clear, dose-dependent escalation in efficacy. By hitting the KRAS pathway from multiple angles, the regimen prevents the cancer from pivoting to alternative signaling pathways—a common cause of failure in earlier KRAS trials.
The Safety Profile
Increased efficacy often comes at the cost of higher toxicity. In KANDLELIT-001, grade 3 or 4 adverse events occurred in 9% of patients on monotherapy, rising to 20% in the doublet group and 42% in the triplet group. While these numbers are higher, Jane Healy, Vice President and Head of Oncology Early Development at Merck Research Laboratories, maintains that the profile is "manageable and reflective of the individual agents," suggesting that the clinical benefits of the triplet therapy currently outweigh the manageable safety risks.
Monitoring the Response: The Role of ctDNA and VAF
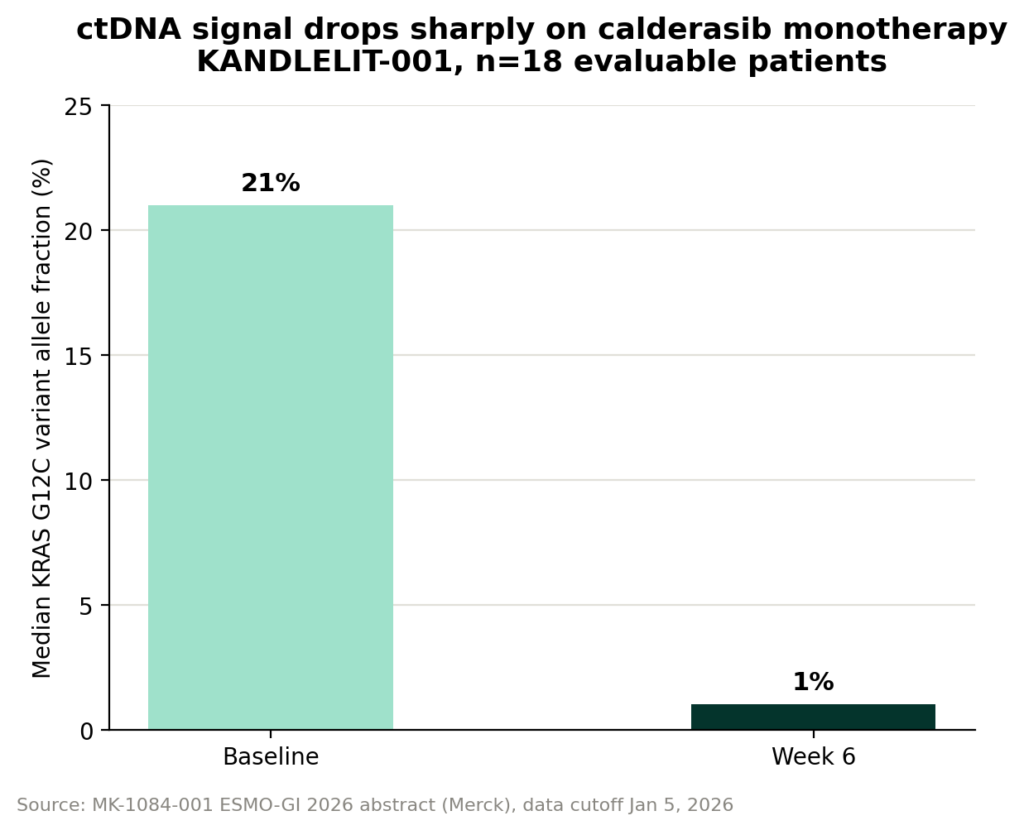
One of the most innovative aspects of the calderasib development program is its heavy reliance on circulating tumor DNA (ctDNA) as a real-time monitor of disease progression.
By measuring the Variant Allele Fraction (VAF)—the percentage of mutant tumor DNA fragments shed into the bloodstream—researchers can track the tumor’s response with precision. In the KANDLELIT-001 study, researchers observed a median VAF reduction of approximately 95% in patients treated with calderasib monotherapy, with levels dropping from 21% at baseline to 1% by week 6.
This approach offers several advantages:
- Speed: Blood draws provide data far faster than traditional radiographic imaging (CT/PET scans).
- Sensitivity: Changes in VAF often precede physical changes in tumor size, allowing clinicians to detect resistance or progression months earlier.
- Dynamic Monitoring: Frequent testing allows for a "fluid" view of the disease, moving away from the "snapshot" approach of quarterly imaging.
Official Perspectives: The Merck Strategy
For Merck, calderasib is more than just a new oncology drug; it is a validation of the company’s "biomarker-first" strategy. Jane Healy emphasizes that the company is leveraging its history with pembrolizumab (Keytruda) to navigate this new landscape.
"Merck actually had the first tumor-agnostic approval for a drug with pembrolizumab," Healy notes. "That was the first time a regulatory agency approved a therapy based on a biomarker status rather than the organ of origin. We are applying that same logic to calderasib."
By enrolling patients with KRAS G12C-mutated solid tumors regardless of whether the cancer started in the colon, lung, or pancreas, Merck is betting that the mutation itself is the primary driver of the tumor’s vulnerability. This "pan-tumor" approach has the potential to streamline drug development, allowing a single drug to secure multiple indications based on shared genomic markers.
Future Implications: Moving to Phase 3
The success of the Phase 1 KANDLELIT-001 trial has paved the way for the pivotal Phase 3 KANDLELIT-012 trial. This study will focus specifically on 1L (first-line) KRAS G12C-mutant colorectal cancer, testing the triplet combination of calderasib, cetuximab, and chemotherapy.
The Path Forward
The oncology community is watching this trial closely for three reasons:
- Standard of Care Shifts: If the 87% ORR seen in treatment-naïve patients holds up in a larger, randomized, controlled Phase 3 setting, it could fundamentally redefine the standard of care for metastatic colorectal cancer.
- Validation of the Triplet Approach: While doublet therapies are becoming more common in KRAS inhibition, triplet therapies remain aggressive. KANDLELIT-012 will determine whether the long-term survival benefits justify the increased toxicities seen in early data.
- The Biomarker-First Model: If calderasib achieves success across diverse tumor types, it will cement the "biomarker-first" regulatory pathway as the dominant model for future precision oncology development, potentially reducing the time it takes for life-saving drugs to reach patients.
A New Era of Precision
The transition from "undruggable" to "highly combinable" marks a coming-of-age for KRAS research. Merck’s commitment to this pathway, reinforced by the high-precision monitoring of ctDNA and a pan-tumor regulatory strategy, positions calderasib at the vanguard of modern oncology.
While the data remains preliminary and requires validation through larger, randomized Phase 3 trials, the trajectory is clear. By focusing on the structural biology of the protein and the reality of cellular signaling pathways, Merck is not just attacking a single cancer—it is building a platform for the next decade of precision medicine. The success of this endeavor will depend on whether the clinical data continues to reflect the promise seen in the laboratory, but for now, the "combinability" thesis remains one of the most compelling narratives in modern drug discovery.