The transition from a routine medical screening to a life-altering diagnosis is often described by patients as a moment where time both freezes and accelerates. For Alice Tawil, that moment arrived in February 2025. What began as a standard mammogram quickly evolved into a rigorous battle against Triple Negative Breast Cancer (TNBC), a particularly aggressive subtype of the disease.
Her journey, documented throughout the spring and summer of 2025, serves as a profound case study in the intersection of modern oncology, the psychological burden of life-threatening illness, and the critical role of specialized support organizations. Tawil’s experience highlights not only the clinical realities of cancer treatment but also the emotional resilience required to navigate significant family milestones—specifically her son’s engagement and wedding—while undergoing debilitating therapy.
Main Facts: The Diagnosis and Clinical Profile
In early 2025, Alice Tawil underwent a routine mammogram that identified a suspicious mass. Subsequent biopsies confirmed the presence of a tumor. While initial assessments suggested a relatively straightforward path involving a lumpectomy followed by localized treatment, the pathology report revealed a more complex reality: Stage 1 Triple Negative Breast Cancer.
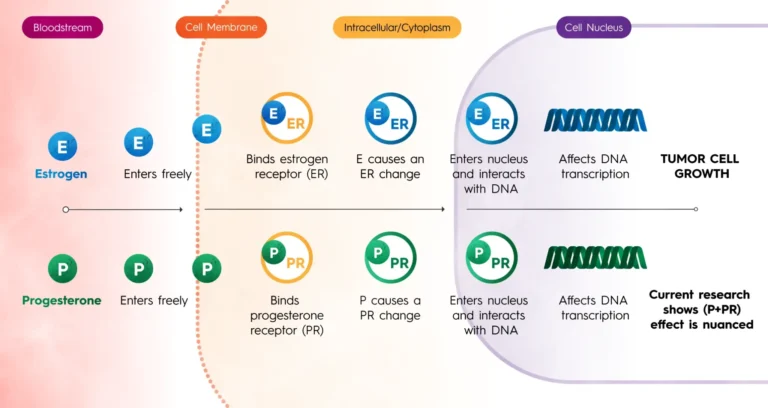
TNBC is defined by the absence of three primary receptors known to fuel most breast cancers: estrogen receptors (ER), progesterone receptors (PR), and the human epidermal growth factor receptor 2 (HER2). Because the cancer cells lack these receptors, traditional hormone therapies and HER2-targeted drugs are ineffective. This diagnostic profile necessitates a more aggressive systemic approach, typically involving heavy chemotherapy, even in early-stage cases like Tawil’s.
The clinical facts of Tawil’s case include:
- Diagnosis Date: February 2025.
- Pathology: Stage 1 Triple Negative Breast Cancer (TNBC).
- Surgical Intervention: Initial lumpectomy to remove the primary tumor.
- Systemic Treatment: Four rounds of intensive chemotherapy.
- Localized Treatment: 15 sessions of radiation therapy.
- Timeline of Recovery: Treatment concluded in September 2025.
The Chronology of a Crisis: From Screening to Celebration
The timeline of Alice Tawil’s journey is a testament to the rapid pace of oncological intervention.
February – March 2025: Detection and Initial Surgery
Following the suspicious finding in February, Tawil moved quickly into the diagnostic phase. The confirmation of a small tumor led to a scheduled lumpectomy. At this stage, the patient’s expectation was centered on a "standard" recovery involving surgery and perhaps mild medication. However, the post-surgical pathology report—which identified the triple-negative status—altered the trajectory of her care. Her oncology team shifted the protocol to include systemic chemotherapy to mitigate the high risk of recurrence associated with TNBC.
Spring 2025: The Intersection of Joy and Illness
As Tawil began her chemotherapy regimen, her personal life reached a significant milestone: her son’s engagement. This period highlights a common struggle for cancer patients—the desire to maintain a sense of normalcy and joy for the sake of family. Tawil chose to keep her diagnosis private, sharing the news only with her immediate family. She successfully hosted an engagement party at her home, balancing the physical toll of treatment with the emotional demands of a celebration.
Summer 2025: The Rigors of Treatment
The summer months were defined by four rounds of chemotherapy followed by 15 sessions of radiation. This period represented the "difficult moments" Tawil described, including the distressing experience of hair loss—a side effect that often serves as the most visible marker of the disease. During this phase, Tawil integrated the support of Sharsheret, a national non-profit organization, into her daily life.
September 2025: Completion and the Wedding
Tawil’s treatment concluded in early September 2025. This was a critical deadline, as her son’s wedding was scheduled for the following week. Finishing 15 rounds of radiation just seven days before a major life event allowed Tawil to transition from "patient" to "Mother of the Groom," a transition she credits to both medical success and psychological support.
Supporting Data: Understanding the TNBC Challenge
Tawil’s diagnosis of Triple Negative Breast Cancer places her in a category that accounts for roughly 10% to 15% of all breast cancer cases. To understand the gravity of her journey, one must look at the data surrounding this specific subtype.
- Aggressive Nature: TNBC is known to grow and spread faster than other types of breast cancer. It also has a higher likelihood of recurrence within the first three to five years following diagnosis compared to hormone-receptor-positive cancers.
- Treatment Limitations: Because TNBC does not respond to hormonal therapy (like Tamoxifen or Aromasin) or targeted HER2 drugs (like Herceptin), chemotherapy remains the primary systemic treatment. This explains why Tawil, despite having a "small tumor" and "Stage 1" diagnosis, was still required to undergo a rigorous four-round chemo regimen.
- Demographics and Genetics: While TNBC can affect anyone, it is more prevalent in women under 40, African American women, and those with a BRCA1 genetic mutation. Support organizations like Sharsheret specifically focus on these high-risk populations, particularly within the Jewish community where BRCA mutations are more common.
- Survival Rates: The five-year survival rate for localized TNBC (Stage 1) is approximately 91%. Early detection, such as Tawil’s routine mammogram, is the single most important factor in achieving these positive outcomes.
Official Responses and the Role of Sharsheret
A critical component of Alice Tawil’s recovery was her engagement with Sharsheret, a leading organization dedicated to supporting Jewish women and families facing breast and ovarian cancer.

The Sharsheret Support Model
Upon the recommendation of a friend, Tawil connected with the organization, which provided a multi-layered support system. According to the organization’s mission, they aim to offer "culturally relevant" support that addresses the unique concerns of Jewish families, though their services are open to all.
Tawil was paired with a dedicated social worker, a move that clinical studies suggest significantly improves patient outcomes by reducing anxiety and depression. The "care packages" mentioned by Tawil—containing educational resources, healthy cookbooks, exercise bands, and comfort items like blankets—are part of Sharsheret’s "Best Face Forward" and "Thriving and Surviving" programs. These programs are designed to address the holistic needs of the patient beyond the clinical administration of drugs.
Expert Perspectives on Holistic Care
Oncologists increasingly recognize that clinical treatment (surgery, chemo, radiation) is only one half of the battle. The "official response" from the medical community regarding cases like Tawil’s emphasizes the necessity of psychosocial intervention.
"The physical side effects of TNBC treatment are grueling," says oncology experts. "But the psychological impact of losing one’s hair and facing a high-recurrence diagnosis while trying to maintain family roles can be equally debilitating. Organizations that provide a bridge between the hospital and the home are essential for long-term recovery."
Implications: The Importance of Early Detection and Support
Alice Tawil’s journey carries several broader implications for public health and patient advocacy.
1. The Criticality of Routine Screening
Tawil’s cancer was caught during a routine mammogram. Given the aggressive nature of Triple Negative Breast Cancer, a delay of even a few months could have resulted in the cancer progressing to Stage 2 or 3, necessitating even more invasive treatment and lowering the statistical probability of a cure. Her case reinforces the medical consensus that regular screening is the most effective tool in the fight against aggressive cancer subtypes.
2. The Power of "Social Prescribing"
The recommendation by a friend to join Sharsheret is an example of "social prescribing"—referring patients to non-clinical services to improve health and well-being. Tawil’s reliance on her social worker and the provided educational resources suggests that medical teams should more aggressively integrate non-profit support services into the standard care plan.
3. Balancing Life and Illness
Tawil’s decision to host an engagement party and attend a wedding at the bookends of her treatment highlights the "invisible" struggle of many cancer patients. The ability to maintain a public persona of health while undergoing private physical trauma requires immense emotional labor. Tawil’s story emphasizes the need for support systems that help patients manage these social and familial expectations.
4. The Path Forward for TNBC Research
While Tawil’s treatment was successful, her journey underscores the need for continued research into TNBC. Currently, chemotherapy remains a "blunt instrument" for this subtype. Future implications for patients like Tawil involve the development of immunotherapy and more refined targeted treatments that could one day replace the intensive chemo/radiation cycle she endured.
Conclusion
Alice Tawil completed her treatment in September 2025, just in time to witness her son’s wedding—a milestone that served as a beacon of hope throughout her darkest months. Her journey from a February mammogram to a September celebration is a narrative of medical efficiency, personal fortitude, and the vital safety net provided by community organizations.
By sharing her story, Tawil offers a roadmap for others facing a similar diagnosis: the importance of early detection, the courage to accept help, and the possibility of emerging from a grueling year of treatment in time for life’s most joyous moments. Her experience stands as a testament to the fact that while a cancer diagnosis changes a life, with the right support, it does not have to define it.