Editorial Note: Originally published on January 13, 2026, this report has been continuously updated—most recently on July 1, 2026—to reflect the latest developments in the U.S. government’s global health strategy.
Introduction: A Strategic Pivot
On September 18, 2025, the United States government unveiled its "America First Global Health Strategy," a foundational document signaling a departure from traditional models of international health assistance. For decades, U.S. foreign aid in the health sector functioned largely as a donor-recipient paradigm. The new strategy, however, replaces this with a framework of bilateral cooperation defined by "co-investment" and a clear, time-bound path toward local self-reliance.
Central to this initiative are formal Memorandums of Understanding (MOUs) signed between the U.S. and partner nations. These five-year roadmaps (2026–2030) establish a structured transition, where the U.S. gradually decreases its financial footprint as partner countries pledge to scale up their domestic health spending. This shift aims to move beyond temporary relief toward the creation of resilient, durable, and locally owned health systems.

Chronology of the New Strategy
The implementation of this policy has been deliberate, moving from high-level strategic planning to granular, nation-specific agreements.
- September 18, 2025: The State Department officially releases the America First Global Health Strategy, formalizing the move toward bilateral co-investment models.
- Late 2025: The first wave of MOUs is signed. Diplomatic missions begin the process of aligning U.S. aid portfolios with the new five-year transition goals.
- January 2026: The inaugural release of the tracking dashboard provides the public with a transparent view of the emerging bilateral agreements.
- July 2026: Updated data shows an expansion of the program, with more countries formalizing their commitments to increasing domestic health budgets in exchange for continued, albeit tapering, U.S. technical support.
- Late 2026 (Forthcoming): Full-scale implementation of the 2026–2030 transition plans is slated to begin, marking the start of the first phase of the "co-investment" timeline.
Analyzing the Data: Tracking the Transition
To ensure transparency, a comprehensive tracker has been established to monitor the evolution of these agreements. The data, sourced from U.S. embassies, State Department press releases, and partner ministries, is organized into several key metrics:
1. Funding Trajectories
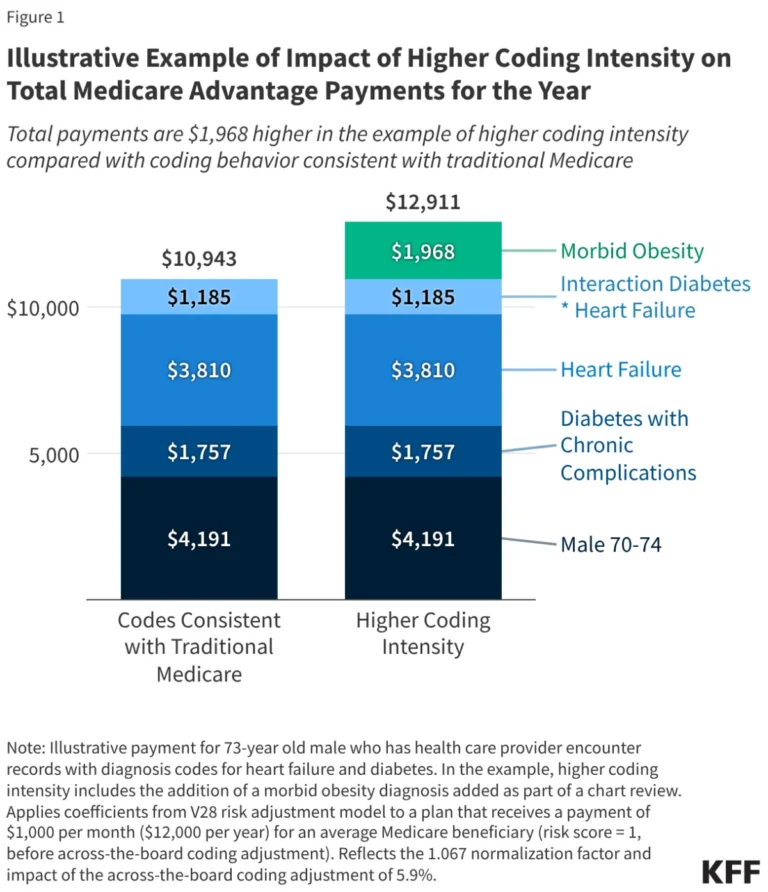
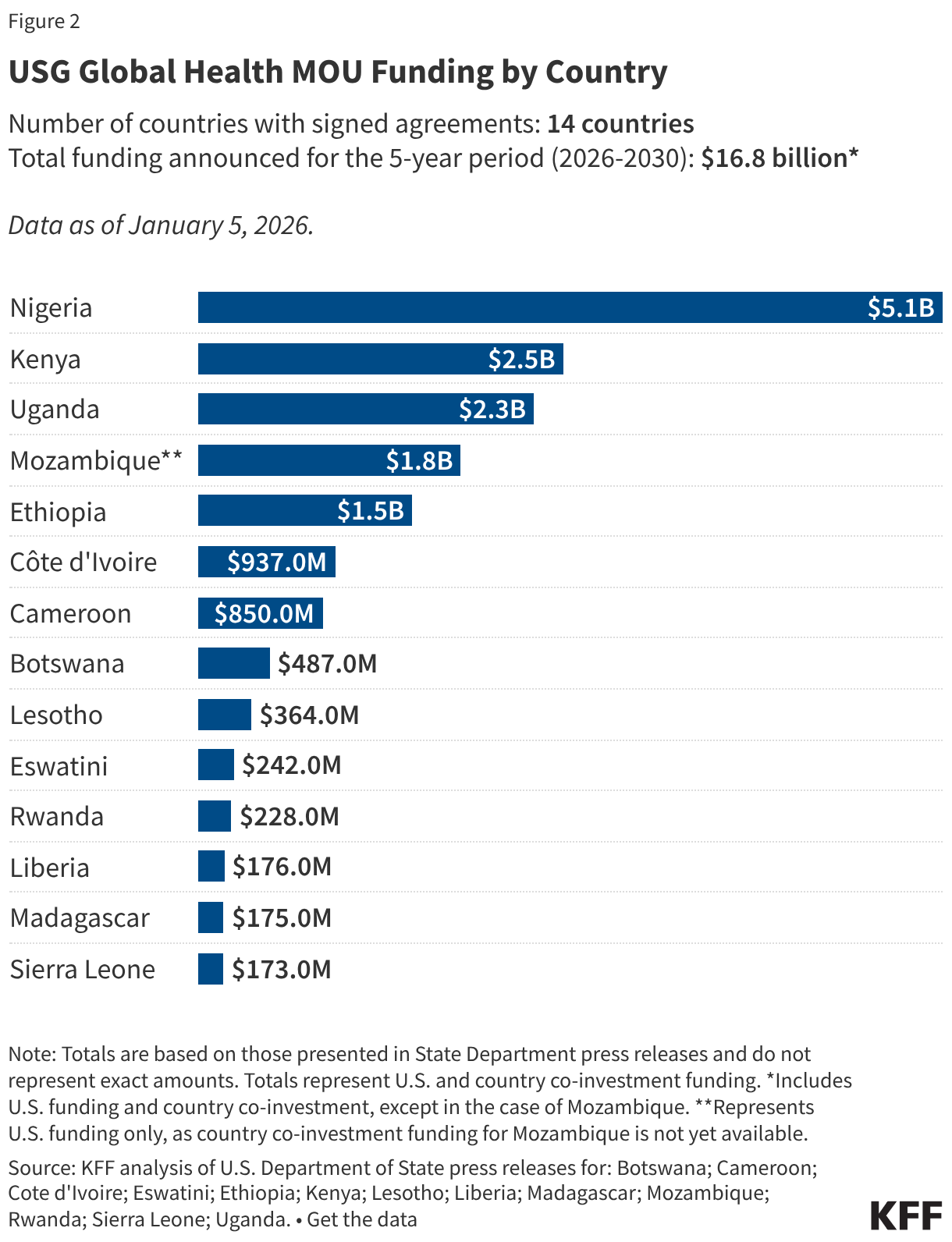
The core of the strategy is the reduction of U.S. financial dependence. By comparing historical aid levels with proposed funding under the 2026–2030 MOUs, observers can visualize the anticipated "glide path" toward domestic sovereignty. The grouped bar charts provided in the tracker illustrate this narrowing gap, where the U.S. contribution descends while the domestic co-financing share rises proportionally.

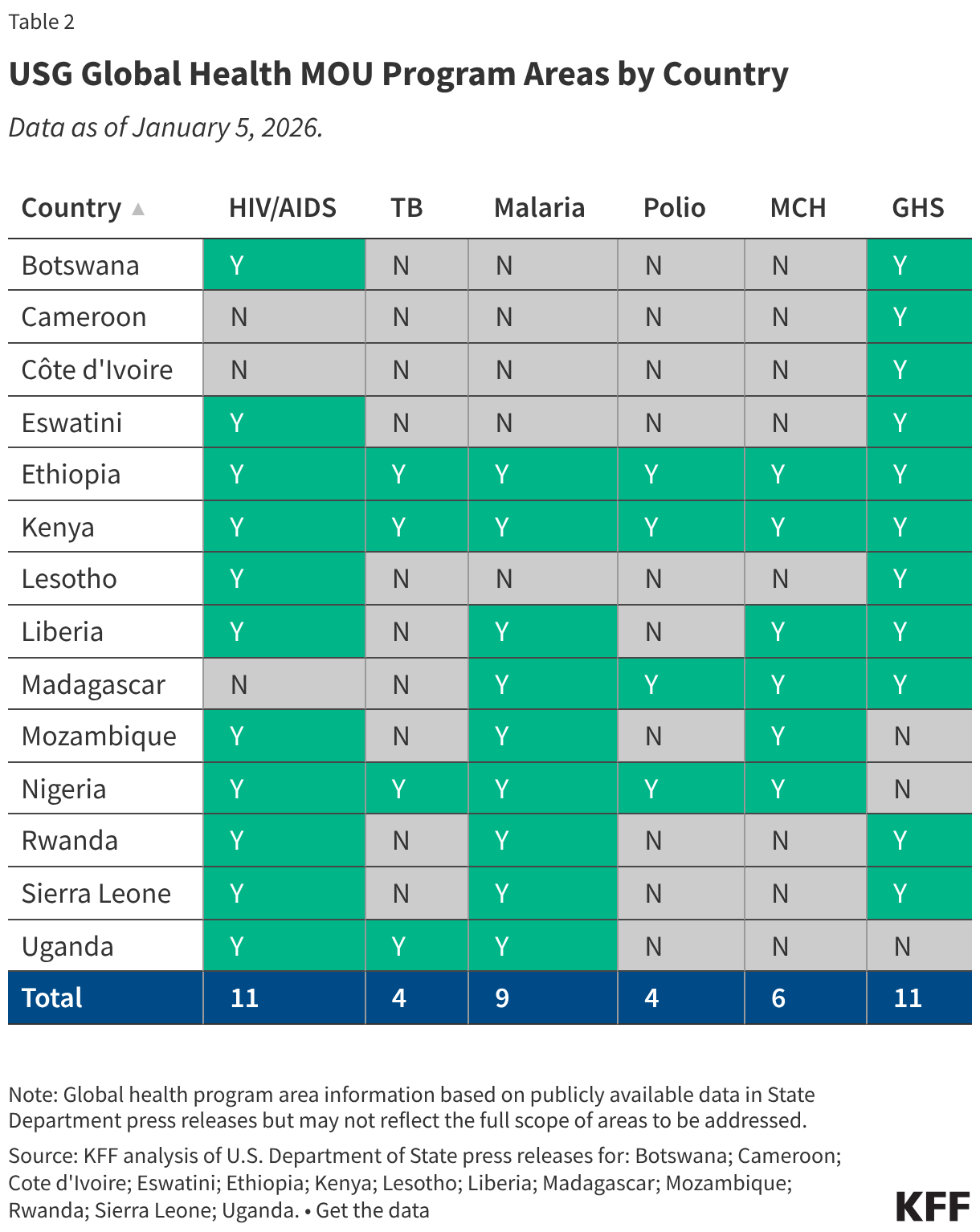
2. Programmatic Focus
While the overarching goal is structural resilience, the MOUs specify technical areas of cooperation. Using keyword analysis, the tracker categorizes agreements based on:
- Global Health Security (GHS): Outbreak preparedness, pandemic response, and threat detection.
- Primary Healthcare: Strengthening foundational infrastructure.
- Maternal and Child Health: Ongoing legacy programs transitioning to local management.
- Infectious Disease Control: HIV/AIDS, Malaria, and Tuberculosis initiatives.
3. Geographic Scope
The choropleth maps provided in the official tracker highlight a global footprint, emphasizing that the strategy is not limited to a single region but is being tailored to diverse geopolitical landscapes, from Southeast Asia to Sub-Saharan Africa and Latin America.
Official Responses and Diplomatic Positioning
The reception of the "America First Global Health Strategy" has been nuanced. U.S. officials maintain that the strategy is a necessary evolution of global health diplomacy.

"We are not abandoning our partners," a spokesperson for the State Department stated during a recent briefing. "We are evolving our relationship from one of aid dependency to one of strategic partnership. By requiring a domestic co-investment, we are ensuring that the health infrastructure we build today survives the withdrawal of U.S. funding tomorrow."
In contrast, some international health advocates have expressed concern regarding the feasibility of these targets. Critics point to the economic volatility of many partner nations, arguing that the five-year window for increasing domestic spending may be overly optimistic in the face of inflationary pressures, debt crises, and competing national security priorities.
However, partner governments have largely signaled a willingness to engage. Many Ministries of Health view the MOUs as a mechanism to formalize their own domestic political commitments to health, using the U.S. agreement as leverage to secure increased budget allocations from their own national treasuries.
Implications: What This Means for Global Health
The shift toward "Country Ownership" carries profound implications for the international development landscape.
For U.S. Foreign Policy
The strategy aligns global health with the broader "America First" diplomatic framework. By emphasizing fiscal responsibility and measurable outcomes, the administration aims to build a sustainable model that can withstand domestic political scrutiny in the U.S. regarding foreign aid expenditures.
For Global Health Security
The emphasis on GHS is perhaps the most critical component. The post-2025 reality requires that every nation possesses a baseline of laboratory capacity, disease surveillance, and rapid response capabilities. By codifying these requirements in MOUs, the U.S. is effectively creating a standardized international requirement for health security, treating it as a prerequisite for bilateral cooperation.
For Developing Nations
The requirement to increase domestic health spending will force a reallocation of resources within partner countries. This is expected to trigger a shift in domestic policy-making, where public health becomes a core pillar of national economic planning rather than a peripheral social issue funded by international NGOs and U.S. agencies.
Methodology: Ensuring Data Integrity
To maintain the credibility of this tracking initiative, the methodology relies on a multi-tiered approach:
- Source Verification: Data is culled exclusively from official government documents. In instances where the full text of an MOU is public, researchers extract annual funding data directly. Where texts remain confidential, press releases serve as the primary proxy.
- Keyword Categorization: Program areas are determined by explicit mentions in MOU summaries. For "Global Health Security," the criteria include explicit mentions of GHS or, alternatively, descriptions of outbreak preparedness, diagnostic capacity, and border health security.
- Limitations: The tracker acknowledges inherent limitations. Because not all MOUs are public, some data points are based on initial announcements, which may be subject to future renegotiation. Furthermore, the "co-investment" percentages are based on projected budgets; the actual execution of these budgets will be monitored as annual reports become available through 2030.
Future Outlook: Moving Toward 2030
As we look toward the 2030 deadline, the success of this strategy will be measured not by the amount of aid delivered, but by the maturity of the health systems left in its wake. If the strategy succeeds, the U.S. will have successfully institutionalized a model of "graduation" for partner nations. If it falters, it risks creating a "funding cliff" where essential health services are dismantled due to a lack of domestic fiscal capacity.
The ongoing updates to this tracker will remain essential for policymakers, researchers, and citizens alike. As more agreements are signed and the first full year of implementation concludes, the data will provide an empirical window into whether this ambitious transition can truly deliver on its promise of a more resilient, self-sustaining global health architecture.
For now, the world watches as the U.S. moves into the second year of this experiment—a period that will prove crucial in determining whether this new bilateral paradigm represents a permanent shift in the nature of international development assistance.
Data References:
- For real-time updates and interactive charts, please refer to the official State Department Global Health Portal.
- Methodological inquiries regarding the keyword search criteria can be directed to the technical research team managing the dashboard.