The landscape of breast cancer is shifting. Once considered a disease primarily affecting post-menopausal women, an increasing number of women are now being diagnosed in their 20s, 30s, and early 40s—prime years for starting or expanding families. This demographic shift has brought the field of "oncofertility" to the forefront of oncology. For these younger patients, a breast cancer diagnosis carries a dual burden: the immediate threat to their life and a potential long-term threat to their dreams of biological motherhood.
Recent research, including landmark studies supported by the Breast Cancer Research Foundation (BCRF), provides a beacon of hope. While treatments like chemotherapy and hormone therapy present significant challenges to reproductive health, advancements in fertility preservation and a deeper understanding of treatment timing are allowing more survivors than ever to conceive healthy children.
Main Facts: The Biological Impact of Treatment on Reproduction
It is a common misconception that breast cancer itself causes infertility. In reality, breast cancer rarely affects the reproductive organs—such as the uterus or fallopian tubes—or the endocrine glands responsible for hormone production. Instead, the very treatments designed to save a woman’s life are the primary culprits behind reproductive challenges.
The Mechanism of Infertility
Fertility is primarily compromised when treatments damage the ovaries or disrupt the delicate hormonal balance required for ovulation and pregnancy. The extent of this impact is highly individualized, dictated by the patient’s age, baseline ovarian reserve, the specific drugs used, and the duration of the treatment.
- Chemotherapy: This remains the most significant risk. Certain agents, particularly alkylating agents like cyclophosphamide, are "gonadotoxic." They can deplete ovarian follicles—the sacs containing immature eggs—leading to primary ovarian insufficiency (POI) or early menopause.
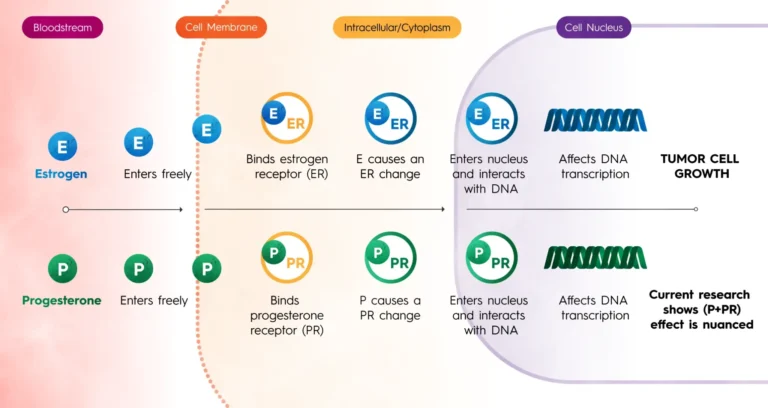
- Hormone Therapy: Used for hormone receptor-positive (ER+) cancers, drugs like tamoxifen do not typically kill eggs but suppress the hormonal signals needed for pregnancy. Because these treatments often last five to ten years, the primary risk is the "age factor"—by the time treatment ends, a woman’s natural fertility may have declined significantly.
- Radiation: While localized breast radiation is generally safe for fertility, any "scatter" radiation to the pelvic region can potentially damage the ovaries.
Chronology: From Diagnosis to Post-Treatment Conception
The journey for a young breast cancer patient involves a complex timeline where medical decisions must be made rapidly, often within days of a biopsy result.
Phase 1: The Preservation Window (Pre-Treatment)
Immediately following diagnosis, a critical window exists before systemic treatment begins. This is when fertility preservation must occur. Patients typically undergo a two-to-three-week cycle of ovarian stimulation, similar to IVF, to harvest eggs or embryos. If chemotherapy must start immediately, this window is shortened, necessitating alternative methods like ovarian tissue cryopreservation.
Phase 2: The Active Treatment Years
During chemotherapy, some patients receive GnRH agonists (ovarian suppression) to "shut down" the ovaries temporarily, potentially shielding them from the toxic effects of the drugs. Following chemotherapy, many patients transition to years of hormone therapy.
Phase 3: "The Pause" (The POSITIVE Trial Model)
For years, women with ER+ cancer were told they must finish five years of hormone therapy before trying to conceive. However, the groundbreaking POSITIVE trial (Pregnancy Outcome and Safety of Interrupting Systemic Therapy for Women with Endocrine Responsive Breast Cancer) has changed the chronology. The study demonstrated that many women can safely pause their hormone therapy after 18 to 30 months to attempt pregnancy, returning to treatment after childbirth.
Phase 4: Post-Treatment Family Building
Once treatment is complete (or safely paused), patients enter the conception phase. This may involve natural conception or the use of previously frozen eggs and embryos. Monitoring for recurrence remains a priority during this period, requiring close collaboration between oncologists and reproductive specialists.
Supporting Data: Statistics and Success Rates
Recent clinical data provides a more optimistic outlook than was available a decade ago. A pivotal study published in the journal Cancer in 2023 followed women diagnosed at age 40 and younger with Stage 0 to Stage III breast cancer. The results were encouraging: the majority of participants who attempted to get pregnant were successful, and most achieved a live birth.
Key Data Points:
- Ovarian Insufficiency Rates: A meta-analysis of five major studies involving younger breast cancer patients treated with chemotherapy showed a POI rate of 31%. While significant, it indicates that nearly 70% of women did not experience early menopause.
- The Protective Power of GnRH: In patients who used ovarian suppression (GnRH agonists) during chemotherapy, the rate of POI dropped significantly to approximately 14%.
- Safety of Stimulation: Concerns that the high estrogen levels required for egg harvesting might "feed" a cancer have been largely mitigated. A study co-authored by BCRF investigator Dr. Ann Partridge found no difference in invasive disease-free survival at five years between women who underwent fertility preservation and those who did not.
- Age as a Predictor: Statistics consistently show that women treated before age 35 have higher post-treatment pregnancy rates, largely due to a more robust baseline egg count.
Official Responses and Expert Perspectives
The medical community has shifted its stance from a "cancer-first, family-later" approach to an integrated model of care. Leading organizations like the American Society of Clinical Oncology (ASCO) and the American Society for Reproductive Medicine (ASRM) now mandate that fertility discussions occur as soon as possible after diagnosis.
The Role of BCRF and Dr. Ann Partridge
Dr. Ann Partridge, a leading BCRF investigator and founder of the Program for Young Women with Breast Cancer at Dana-Farber Cancer Institute, has been instrumental in this shift. Her work emphasizes that "knowledge is power." Dr. Partridge’s leadership in the POSITIVE trial has provided the clinical evidence necessary for doctors to support patients who wish to interrupt treatment for pregnancy.
"We are seeing that for many women, having a child after breast cancer is not just a dream but a very achievable reality," experts note. The consensus among oncology and fertility specialists is that multidisciplinary care—where the oncologist and the reproductive endocrinologist are in constant communication—is the gold standard for modern treatment.
Psychological and Counseling Recommendations
Both ASCO and ASRM recommend psychological counseling before fertility preservation begins. The emotional toll of making reproductive decisions while processing a cancer diagnosis is immense. Counseling has been shown to improve long-term quality of life and reduce "decisional regret," ensuring that survivors feel at peace with the choices they made during a time of crisis.
Implications: Socioeconomic Realities and Future Directions
While the medical advancements are profound, the implications of these treatments extend into the realms of social justice and economic equity.
The Financial Barrier
Fertility preservation is expensive. A single cycle of egg freezing can cost between $10,000 and $15,000, not including annual storage fees or the eventual cost of implantation. Many insurance plans do not cover these procedures, labeling them "elective" despite their necessity being driven by a medical diagnosis. This creates a tiered system of care where only affluent patients can afford to preserve their future fertility.
Racial and Ethnic Disparities
The implications of these costs are disproportionately felt by women of color. Data indicates that Black and Hispanic women are less likely to be referred to fertility specialists and face greater barriers to accessing care, including difficulty taking time off work and lack of comprehensive insurance coverage. Addressing these disparities is a primary focus for organizations like BCRF, which seeks to ensure that every woman, regardless of her background, has the opportunity to pursue motherhood after cancer.
The Future of Oncofertility
The next frontier in this field involves refining ovarian tissue cryopreservation—a technique currently used primarily for prepubescent girls but increasingly available for adult women who cannot delay treatment even by two weeks. Furthermore, ongoing research is looking into "chemo-protective" drugs that could be administered alongside treatment to prevent ovarian damage entirely.
In conclusion, the intersection of breast cancer and fertility is no longer a "dead end." Through the integration of cutting-edge research, compassionate counseling, and a shift in clinical timelines, the medical community is ensuring that a breast cancer diagnosis does not have to be the end of a woman’s reproductive journey. For the thousands of young women diagnosed each year, these advancements represent more than just medical progress; they represent the preservation of hope and the possibility of a life that continues long after the cancer is gone.