Introduction: A New Paradigm for Medicaid
The landscape of American public health insurance is undergoing a fundamental transformation. With the enactment of the 2025 reconciliation law, federal policy has codified a mandatory work requirement for able-bodied adults enrolled in the Affordable Care Act (ACA) Medicaid expansion group. While the federal government has set a hard deadline of January 1, 2027, for universal compliance, the legislative framework provides states with the flexibility to accelerate this transition.
This shift represents a significant pivot in the philosophy of the Medicaid program, moving it closer to a work-based model traditionally associated with programs like the Supplemental Nutrition Assistance Program (SNAP) or Temporary Assistance for Needy Families (TANF). As states scramble to meet these new federal expectations, a patchwork of implementation strategies has emerged, signaling a complex period of administrative, legal, and social adjustment for millions of beneficiaries across the country.
The Legislative Foundation: Understanding the 2025 Reconciliation Act
The 2025 reconciliation law serves as the bedrock for these changes. By tying Medicaid eligibility to employment or community engagement, Congress has effectively mandated that states verify the work status of expansion-group adults. The legislation is designed to ensure that Medicaid serves as a bridge to self-sufficiency rather than a long-term dependency program.
For policymakers, the challenge lies in the rapid operationalization of these requirements. States must build or adapt robust tracking systems capable of verifying employment hours, managing exemptions, and processing the administrative burden of reporting—a task that historically has proven difficult and costly for state Medicaid agencies.
Chronology of Implementation: A State-by-State Roadmap
While the federal clock is ticking toward January 1, 2027, several states have already signaled their intent to move ahead of the curve. By utilizing State Plan Amendments (SPAs), these jurisdictions are signaling their commitment to the new federal vision.
Early Adopters: The 2026 Timeline
- Nebraska: Leading the charge, Nebraska has announced the most aggressive timeline. Starting May 1, 2026, the state will enforce federal work requirements via a state plan amendment, setting a precedent for other states to follow.
- Montana: Following closely, Montana has scheduled its implementation for July 1, 2026. This transition period is expected to test the state’s capacity to integrate employment data into existing enrollment portals.
- Arkansas: Taking a more cautious, "soft" approach, Arkansas has slated July 1, 2026, as its launch date. Crucially, the state has clarified that while it will begin the compliance process, it will not move to disenroll beneficiaries until the federal deadline of January 1, 2027, effectively allowing for a six-month "grace period" for program participants to adjust to the new rules.
- Iowa: Rounding out the early adopters, Iowa is scheduled to initiate its program on December 1, 2026, just one month before the federal mandate takes full effect.
The Georgia Exception: Navigating 1115 Waivers
Georgia occupies a unique position in this timeline. Following extensive litigation regarding the Biden administration’s attempts to rescind its Medicaid work requirement waiver, Georgia successfully defended its program. As it stands, Georgia is the only state currently operating a work requirement via an 1115 waiver. However, this is a temporary status; the state’s waiver is set to expire on December 31, 2026. Come January 1, 2027, Georgia will be required to align its existing framework with the new federal standard established in the 2025 reconciliation law.
Supporting Data and Administrative Realities
The transition to work requirements is not merely a policy shift; it is a massive data-management endeavor. The effectiveness of these programs will hinge on the accuracy of state labor departments and their ability to interface with Medicaid enrollment systems.
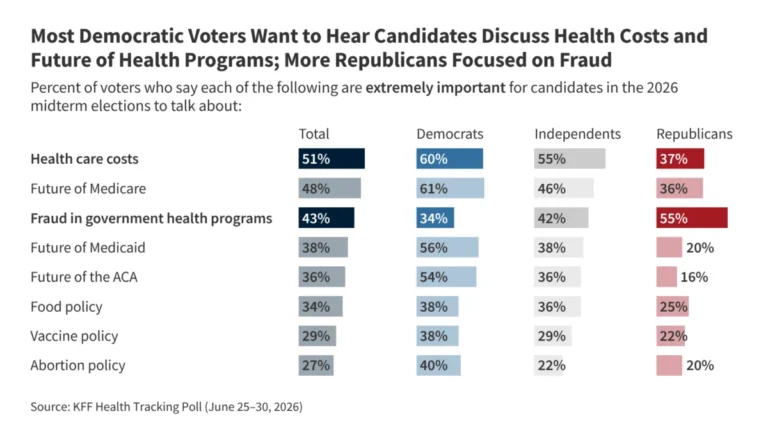
According to current projections from the Kaiser Family Foundation (KFF), the administrative costs associated with implementing these tracking systems are substantial. States must manage complex exemption criteria, including those for caregivers, students, and individuals with disabilities. Without seamless data sharing between agencies, the risk of "administrative churn"—where eligible individuals are disenrolled due to technical glitches or reporting failures—remains high.
Furthermore, the data suggests that while these requirements are aimed at increasing workforce participation, the actual impact on employment rates remains a subject of intense debate among labor economists. In past pilot programs, the majority of individuals who lost coverage were already working but failed to meet the reporting requirements, rather than choosing to remain unemployed.
Official Responses and Political Implications
The move toward universal work requirements has drawn sharp lines between policymakers, advocates, and health policy experts.
Proponents’ Perspectives
Supporters of the 2025 mandate argue that the policy is a matter of fairness and fiscal responsibility. By incentivizing work, they contend, states can move individuals into the labor force, increase tax revenue, and reduce the strain on the Medicaid budget. Supporters often point to the "dignity of work," suggesting that the requirement provides a necessary push for those who are capable of working to find employment in a robust labor market.
Advocates’ Concerns
Conversely, health advocates and civil rights groups have raised alarms regarding the potential for coverage gaps. Critics argue that the reporting requirements disproportionately impact low-income workers, particularly those in the gig economy or seasonal industries with irregular hours. Organizations such as the Center on Budget and Policy Priorities have warned that these requirements could lead to significant enrollment drops, not because beneficiaries have found better employment, but because the bureaucratic hurdles are too high to navigate.
Implications for the Future of Medicaid
As we look toward the 2027 deadline, several critical implications emerge for the American healthcare system:
1. The Death of the 1115 Waiver for Work Requirements
With the federal government codifying these requirements into law, the utility of the 1115 demonstration waiver—which was historically the tool used to test such policies—is effectively diminishing. Because the federal law now mandates these requirements, states no longer need to seek experimental approval to enforce them. This signals a move away from the "laboratory of democracy" approach toward a more uniform, federally directed mandate.
2. Legal Precedents
The resolution of the Georgia litigation serves as a cautionary tale for both state and federal actors. Future legal challenges will likely focus not on the authority to implement work requirements, but on the methods of implementation—specifically, whether the administrative processes are discriminatory or if they violate the "reasonable promptness" requirements of the Medicaid statute.
3. Impact on Health Outcomes
The most significant, yet least understood, implication is the impact on health outcomes. If the mandate results in large-scale disenrollment, what happens to the chronic health conditions of those who lose coverage? Proponents suggest that employment leads to employer-sponsored insurance, while critics fear that the result will be a surge in uncompensated care at emergency rooms, potentially destabilizing rural hospitals that rely on Medicaid reimbursement.
Conclusion: The Road to 2027
The period between now and January 1, 2027, will be defined by administrative preparation and political maneuvering. As Nebraska, Montana, Iowa, and Arkansas lead the way, the rest of the nation will be watching closely. The success of this policy will likely be measured by its ability to balance the goals of workforce participation with the fundamental mission of Medicaid: to provide a safety net for the nation’s most vulnerable populations.
As states finalize their State Plan Amendments, the focus must shift to robust public education campaigns to ensure that beneficiaries understand how to report their hours and maintain their coverage. Without clear communication and a simplified reporting interface, the transition risks becoming an administrative crisis that could overshadow the policy’s stated intent.
Ultimately, the 2025 reconciliation law represents one of the most significant changes to the social safety net in recent history. Whether this change acts as a catalyst for economic mobility or a barrier to healthcare access will be the primary question for researchers, policymakers, and voters for years to come. The era of mandatory work requirements in Medicaid is no longer a prospect; it is a reality, and the nation is now in the midst of a grand-scale transition.