The diagnosis of breast cancer is a life-altering event, but for a growing demographic of younger women, the news carries a double burden: the fight for survival and the potential loss of future motherhood. As the incidence of breast cancer rises among women in their 20s, 30s, and early 40s—ages traditionally associated with family building—the field of "oncofertility" has emerged as a critical component of comprehensive cancer care.
Recent data and clinical trials, including those supported by the Breast Cancer Research Foundation (BCRF), are reshaping the narrative. While treatments like chemotherapy and endocrine therapy have historically posed significant risks to reproductive health, new research suggests that with early intervention and informed decision-making, the dream of having children after cancer is more attainable than ever before.
Main Facts: The Evolving Landscape of Oncofertility
For decades, the primary focus of breast cancer treatment was understandably centered on eradication and survival. However, as survivorship rates have climbed, quality-of-life issues—specifically reproductive health—have moved to the forefront. According to studies published in the journal Cancer, the majority of women diagnosed at age 40 or younger with Stage 0 to Stage III breast cancer are now able to achieve pregnancy and deliver healthy infants following treatment.
The central challenge lies in the fact that breast cancer itself rarely affects fertility directly. Unlike cancers of the reproductive system, breast cancer does not typically damage the ovaries, fallopian tubes, or the uterus. Instead, the "collateral damage" to fertility is usually a byproduct of the life-saving treatments required to treat the disease. Chemotherapy can deplete ovarian reserves, while hormone therapies can necessitate a decade-long delay in childbearing, pushing women past their natural peak fertility years.
The psychological impact of this reality cannot be overstated. Research indicates that concerns about future fertility can influence a patient’s willingness to adhere to treatment protocols, affect their long-term mental health, and even dictate their choice of surgical or systemic interventions.
Chronology: The Patient Journey from Diagnosis to Post-Treatment Conception
The timeline for fertility preservation is often compressed and high-stakes, requiring rapid coordination between oncologists and reproductive specialists.
1. The Immediate Post-Diagnosis Window
The most critical period for fertility preservation occurs between the initial diagnosis and the commencement of systemic treatment. This window, often lasting only a few weeks, is when procedures like egg or embryo freezing must be performed. Because many preservation methods require hormonal stimulation of the ovaries, they must be completed before chemotherapy begins, as the latter can cause immediate and irreversible damage to maturing follicles.
2. The Treatment Phase
During active treatment, which can span months (for chemotherapy and radiation) to years (for hormone therapy), the focus shifts to "ovarian suppression." This involves using medications to put the ovaries into a temporary state of "hibernation" to protect them from the toxic effects of chemotherapy.
3. The Waiting Period and "The Pause"
Historically, survivors were advised to wait at least two years after completing treatment before attempting pregnancy. This was partly to allow the body to clear toxic medications and partly because the risk of recurrence is highest in the first 24 months. However, for women on long-term hormone therapy (which lasts 5–10 years), waiting until the end of treatment often means waiting until they are biologically unable to conceive. This led to the landmark POSITIVE trial, which investigated the safety of temporarily interrupting hormone therapy to allow for pregnancy.
Supporting Data: Understanding the Impact of Treatment
The degree to which fertility is affected depends heavily on the type of treatment, the dosage, and the patient’s age at the time of diagnosis.
Chemotherapy and Ovarian Insufficiency
Chemotherapeutic agents, particularly alkylating agents like cyclophosphamide, are known to be "gonadotoxic." These drugs work by attacking rapidly dividing cells, but they can also destroy the non-dividing primordial follicles in the ovaries. A meta-analysis of five major studies found that approximately 31% of younger breast cancer patients treated with chemotherapy developed Primary Ovarian Insufficiency (POI), a condition where the ovaries stop functioning before age 40. However, the risk is significantly lower for those who use protective measures; only 14% of patients who utilized GnRH agonists (hormonal suppressors) during chemotherapy experienced POI.
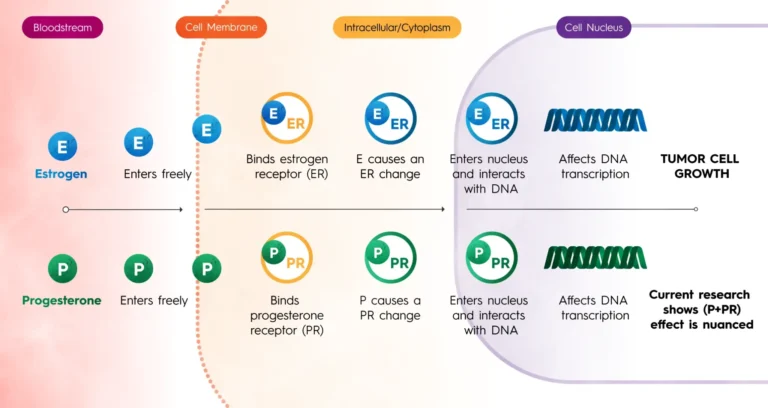
The Impact of Endocrine (Hormone) Therapy
For patients with hormone receptor-positive (ER+) breast cancer, drugs like tamoxifen are standard care. While tamoxifen does not permanently damage the ovaries, it can cause irregular menstrual cycles and is teratogenic (can cause birth defects), meaning women cannot be pregnant while taking it. The 5-to-10-year duration of this therapy is the primary barrier to fertility, as it often spans the remaining years of a woman’s reproductive window.
Radiation Therapy
In contrast to systemic treatments, radiation for breast cancer is typically localized. While "scatter" radiation can occur, modern techniques ensure that the ovaries receive negligible doses. Therefore, standard breast radiation is generally not considered a threat to fertility, provided the radiation is not directed at the pelvic region.
Official Responses and Clinical Guidelines
Leading medical organizations have issued clear mandates regarding the integration of fertility preservation into cancer care. Both the American Society of Clinical Oncology (ASCO) and the American Society for Reproductive Medicine (ASRM) emphasize that fertility preservation should be discussed with every premenopausal patient as early as possible.
The Role of the BCRF and Dr. Ann Partridge
Dr. Ann Partridge, a leading BCRF investigator and co-founder of the Program for Young Women with Breast Cancer at the Dana-Farber Cancer Institute, has been a pivotal voice in this field. Her leadership in the POSITIVE trial provided the scientific community with the first robust evidence that women with early-stage ER+ breast cancer could safely pause their endocrine therapy for up to two years to pursue pregnancy. The study found no short-term increase in recurrence risk among women who took this "pregnancy break," a finding that has revolutionized clinical recommendations for young survivors.
Standard of Care: Cryopreservation
Medical officials now recognize embryo and oocyte (egg) cryopreservation as the gold standard. These procedures have high success rates, though they are dependent on the number and quality of eggs retrieved. For patients who cannot delay treatment even by two weeks, ovarian tissue cryopreservation—once considered experimental—is now an increasingly viable option. This involves surgically removing and freezing ovarian tissue to be reimplanted later.
Implications: Socioeconomic Barriers and Emotional Health
While the medical science of oncofertility has advanced rapidly, the social and economic infrastructure has lagged behind, creating significant disparities in access to care.
Financial Toxicity and Racial Disparities
Fertility preservation is expensive. A single cycle of egg freezing can cost between $10,000 and $15,000, often not covered by insurance. This "financial toxicity" creates a barrier that disproportionately affects women of color. Data shows that Black and Hispanic women face longer delays in seeing reproductive specialists and are less likely to utilize cryopreservation services due to cost and lack of insurance coverage. This gap in care is a growing concern for public health officials who advocate for legislative mandates requiring insurance companies to cover "iatrogenic" (medically induced) infertility treatments.
The Psychological Burden
The intersection of a cancer diagnosis and infertility creates a unique psychological trauma. Patients are forced to make permanent reproductive decisions while in a state of shock and grief. ASCO recommends that all patients interested in fertility preservation receive psychological counseling before beginning treatment. Studies show that patients who receive this support report higher quality of life and lower rates of long-term regret, regardless of whether they successfully conceive.
Future Outlook
The success of the POSITIVE trial and the increasing efficacy of egg freezing have provided a roadmap for the future. The conversation is shifting from "Can we save the patient?" to "How can we ensure the patient has the life they envisioned after cancer?"
As research continues, the goal is to further personalize oncofertility. This includes developing better biomarkers to predict which women are at the highest risk for POI and refining techniques for ovarian tissue transplantation. For the thousands of young women diagnosed with breast cancer each year, these advancements represent more than just medical progress—they represent the preservation of hope and the possibility of a future that includes family.