The landscape of American healthcare finance is bracing for a tectonic shift. Following the enactment of the 2025 reconciliation law, which mandates a $911 billion reduction in federal Medicaid spending over the next decade, policymakers and providers are scrambling to assess the impact of new, stringent restrictions on State Directed Payments (SDPs). These financial mechanisms, once a primary tool for states to bolster provider participation and improve access to care, are now at the center of a federal effort to tighten budgetary control.
A new comprehensive analysis by KFF provides the most granular look yet at the current state of these payments, revealing a complex, multi-billion-dollar ecosystem that sits on the precipice of major regulatory change.
Main Facts: The Scope of Medicaid’s SDP Ecosystem
State Directed Payments allow state Medicaid agencies to mandate that Managed Care Organizations (MCOs) pay specific rates or increase payments to providers for certain services. While MCOs typically negotiate rates directly with hospitals and clinics, SDPs empower states to override these private negotiations to meet public health goals—such as incentivizing care for underserved populations or ensuring financial viability for essential rural hospitals.
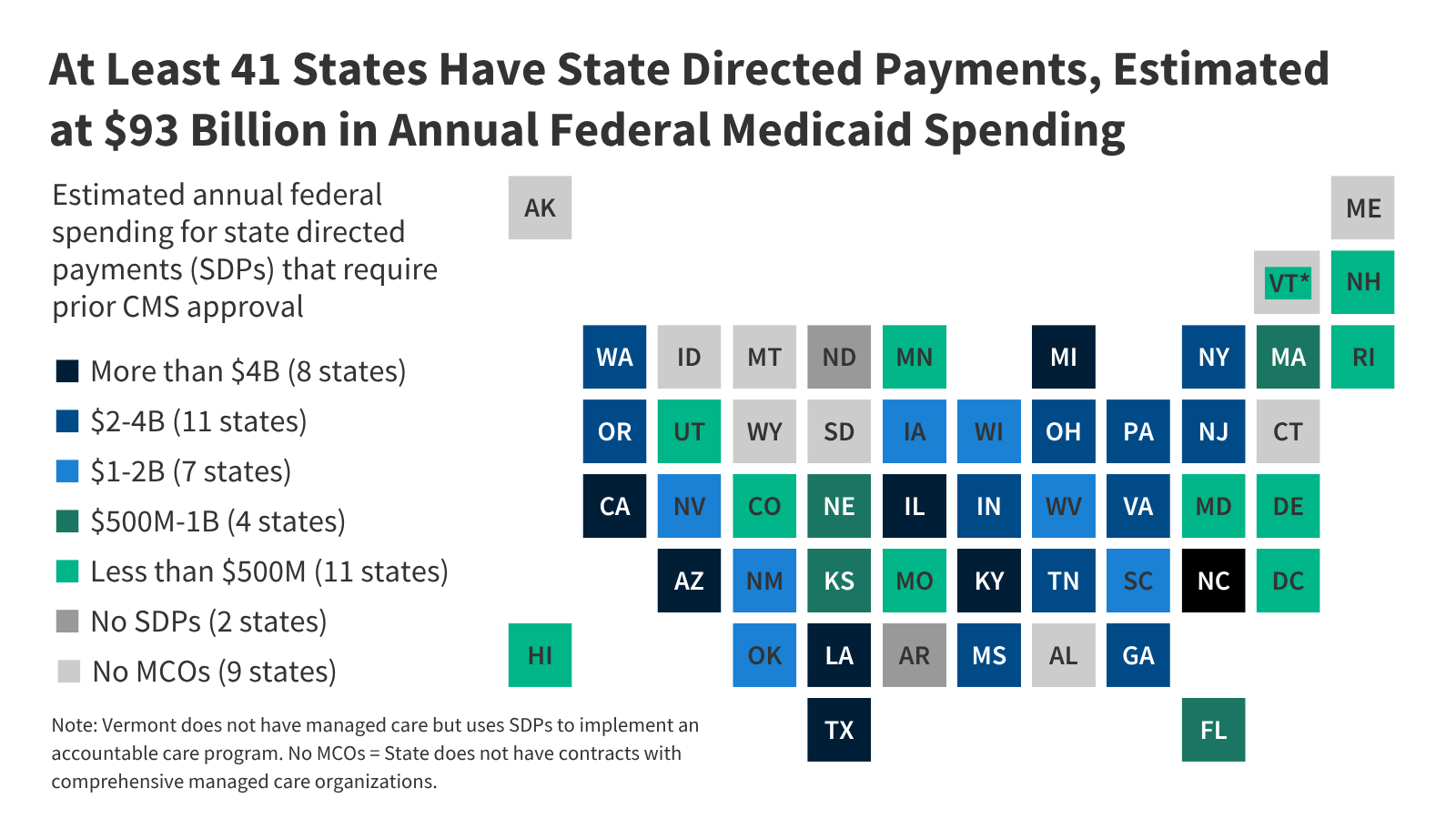
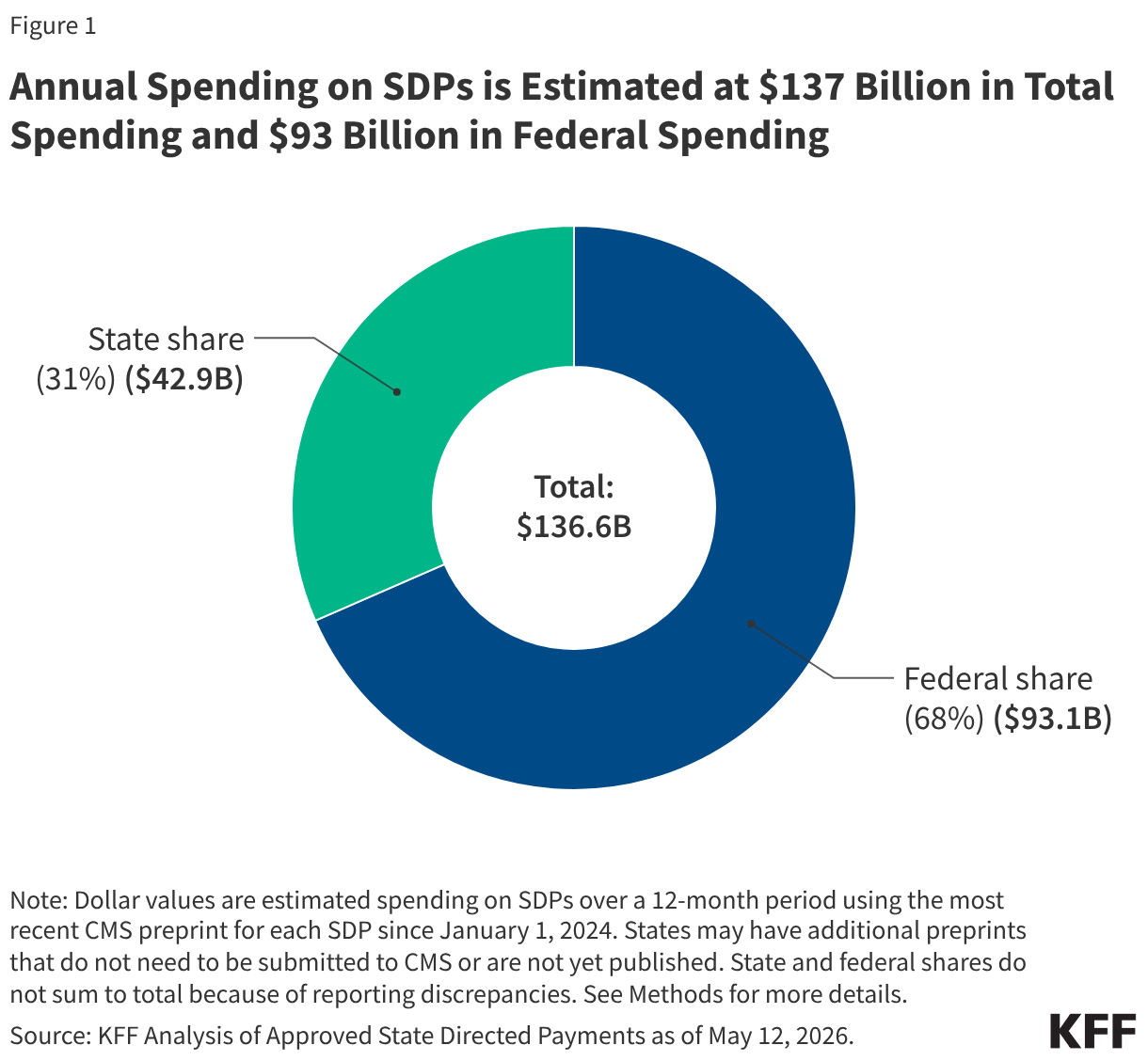
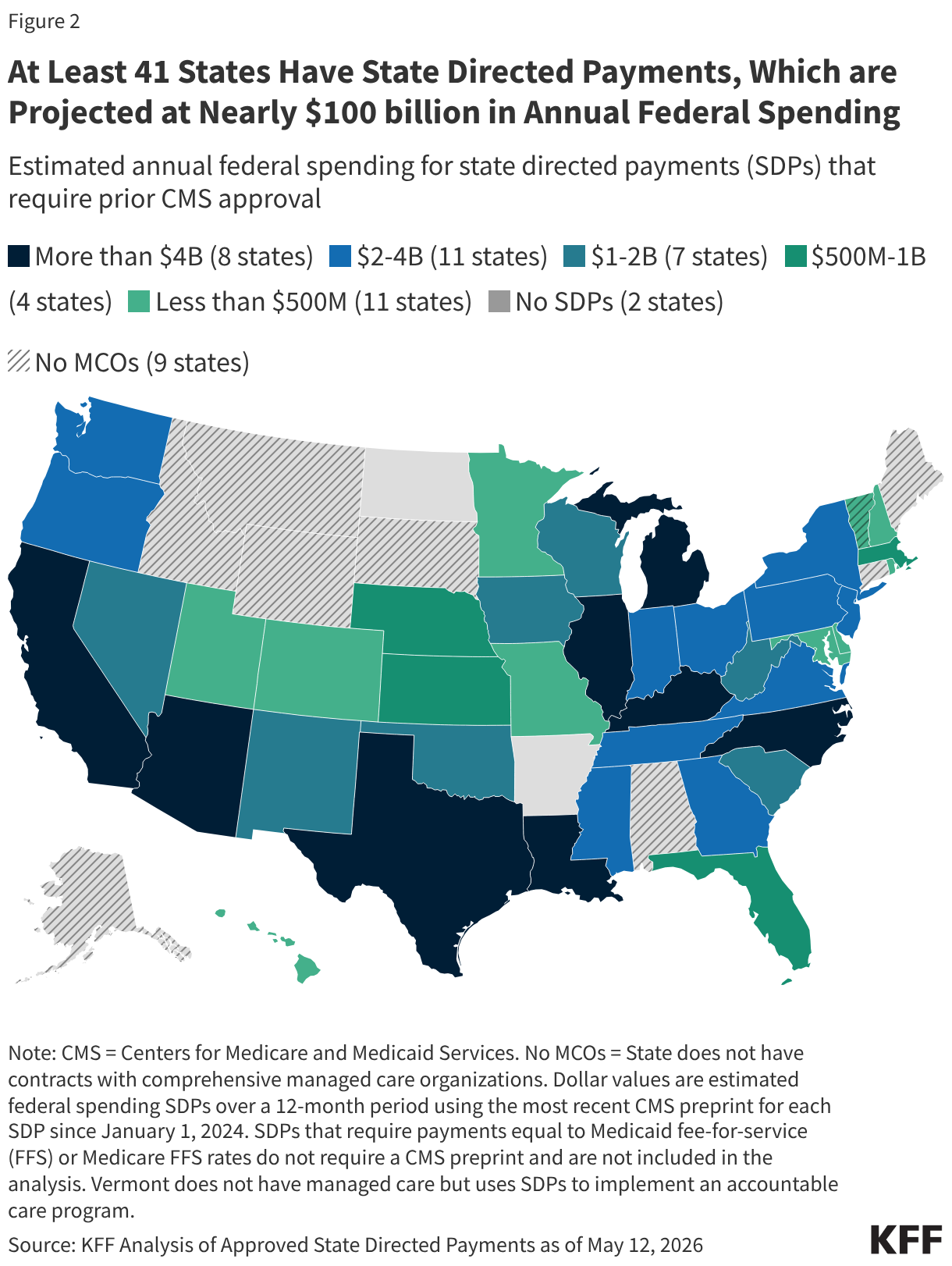
According to KFF’s analysis, which examined 305 approved SDP preprints across 41 states as of May 2026, the current annual spend on these programs is estimated at $137 billion. Of this total, the federal government contributes approximately $93 billion, or roughly 68% of the total financial outlay.
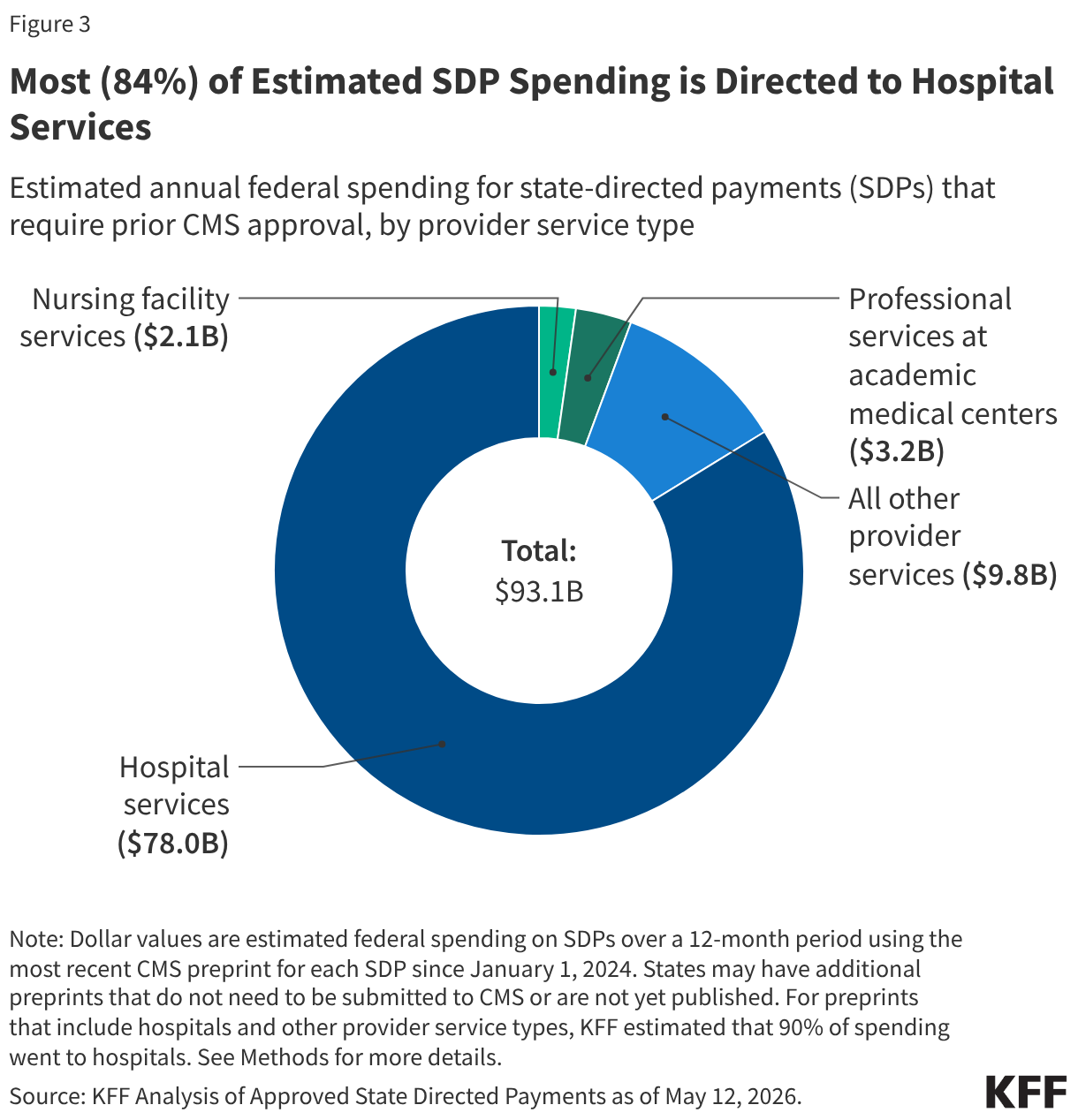
The data reveals a system heavily weighted toward institutional care. An overwhelming 84% of federal dollars channeled through SDPs is directed specifically toward hospital services. Other notable, albeit smaller, beneficiaries include academic medical centers and nursing facilities. This reliance on SDPs as a primary vehicle for hospital funding makes the forthcoming cuts particularly consequential for the nation’s safety-net infrastructure.
Chronology: From Pandemic Flexibility to Fiscal Retrenchment
The evolution of SDPs has been marked by rapid expansion followed by sudden federal scrutiny:
- Pre-2024: States increasingly utilized SDPs to navigate the financial volatility caused by the COVID-19 pandemic, using them to ensure hospital stability while managing the surge in Medicaid enrollment.
- January 1, 2024 – May 2026: The period analyzed by KFF. During this window, states continued to lean on SDPs as a primary method for uniform rate increases, essentially functioning as the managed-care equivalent of traditional fee-for-service supplemental payments.
- May 2026: The Centers for Medicare and Medicaid Services (CMS) released a proposed rule that, in conjunction with the 2025 reconciliation law, signals a definitive pivot toward limiting these payments.
- 2025–2034: The legislative window for the $911 billion in federal Medicaid savings. The reconciliation law introduces strict oversight and caps, forcing states to fundamentally rethink how they finance their managed care programs.
Supporting Data: Complexity and Transparency Gaps
One of the greatest challenges in auditing Medicaid spending is the sheer complexity of financing. Many SDPs are not funded by "new" money; rather, they are backfilled through provider taxes and intergovernmental transfers (IGTs).
For instance, a public hospital might receive a payment boost via an SDP, only to have a portion of that money effectively returned to the state through a transfer to cover the state’s share of the Medicaid match. KFF’s analysis highlights that for many current SDPs, 81% are financed at least in part by these circular fiscal mechanisms. This makes it notoriously difficult to determine the "net" revenue gain for providers.
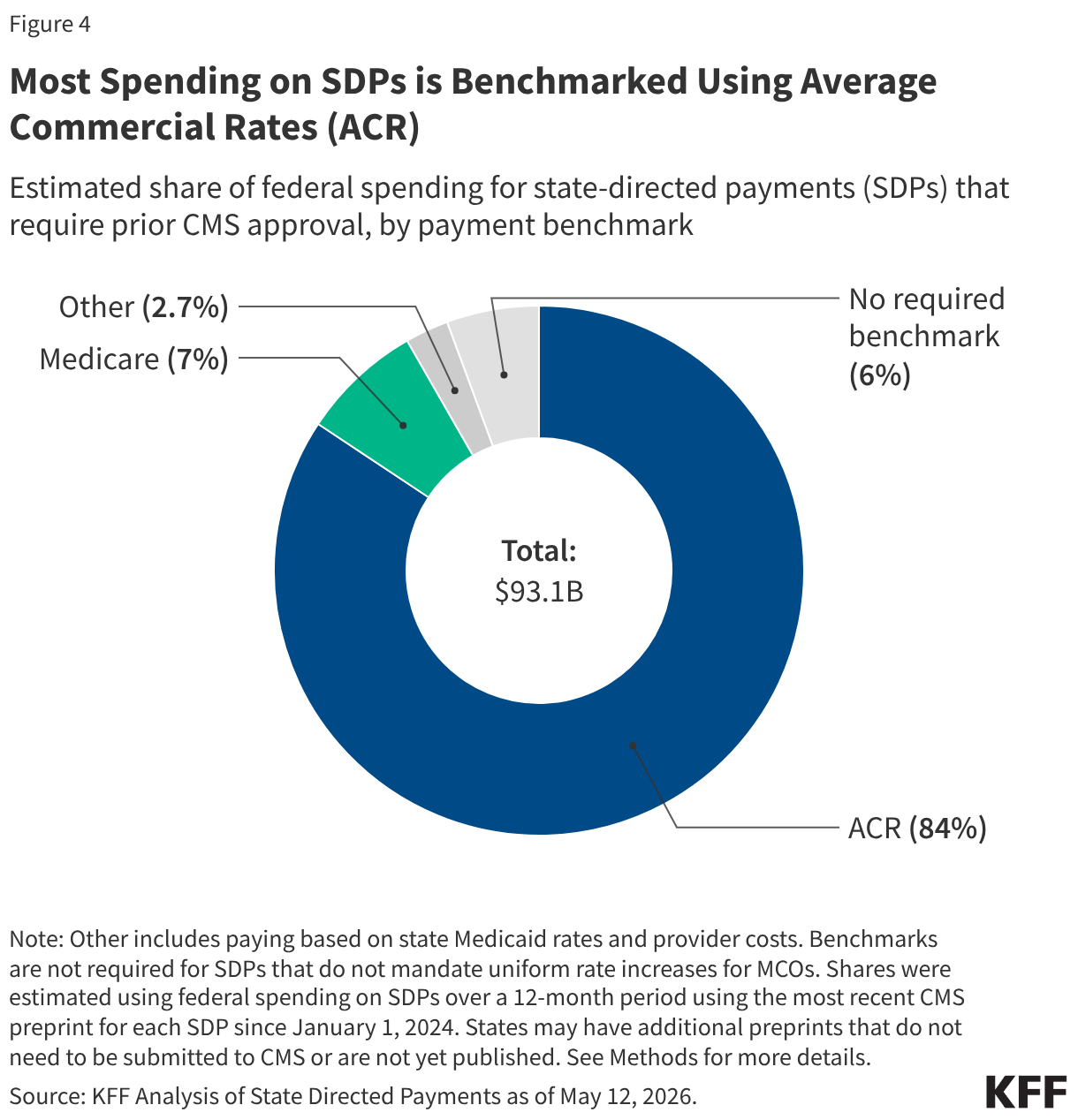
Furthermore, there are significant transparency gaps. The reliance on "preprints"—the application forms states submit to CMS—creates an incomplete picture. Because regulations often exempt payments at Medicare or Medicaid fee-for-service levels from requiring preprints, the public data only reflects a portion of the total financial activity in the sector. Among the SDPs that do report, the reliance on "Average Commercial Rates" (ACR) as a benchmark is dominant, with nearly two-thirds of preprints using ACR to justify their payment levels.
Official Responses and Regulatory Intent
The federal government’s position, articulated through the 2026 proposed rule, emphasizes fiscal sustainability and the need for standardized reporting. CMS has long argued that while SDPs can improve provider participation, they have also been used to mask systemic inefficiencies or to funnel excessive payments to certain facilities without clear evidence of improved health outcomes.
State officials, however, remain concerned. For many states, the ability to direct payments is the only lever they have to prevent a "collapse" of provider networks. In states like Vermont, which utilizes an accountable care organization (ACO) model, the SDP serves as a critical bridge to value-based care, transitioning providers away from volume-based incentives. The concern among state leaders is that if the federal government enforces rigid, one-size-fits-all limits on SDPs, they may inadvertently force providers to exit the Medicaid market, thereby reducing access for the very enrollees the program is designed to serve.
Implications: A High-Stakes Future for Healthcare Access
The implications of the 2025 reconciliation law are profound, affecting every stakeholder in the Medicaid value chain:
For States: A Budgetary Balancing Act
States are facing a "double squeeze." They must navigate reduced federal contributions while simultaneously managing rising costs for care. The reduction in federal support for SDPs will likely force states to either increase their own general fund expenditures—an unlikely prospect given current budget constraints—or renegotiate the terms of their MCO contracts, potentially leading to lower rates for providers.
For Providers: The End of the "Supplemental" Era
Hospitals, particularly those that rely heavily on Medicaid for their patient mix, may face a significant revenue shortfall. The reliance on SDPs to reach commercial-level payment rates has become a staple of hospital finance. If these payments are capped or restricted to lower benchmarks, many facilities may struggle to maintain specialized services, such as emergency care, trauma units, and behavioral health clinics, which are often the first to be cut when supplemental funding dries up.
For Enrollees: Risks to Network Adequacy
The ultimate impact will be felt by the millions of Medicaid beneficiaries. If providers are forced to drop out of managed care networks because reimbursement rates are no longer sustainable, enrollees may face longer wait times, travel further for care, or experience a decline in the quality of services available in their local communities. The "access to care" promise of Medicaid, which was the original justification for allowing SDPs, may be compromised by the very policies intended to save the federal budget.
The Path Forward: Data-Driven Decision Making
As the industry moves toward the 2034 horizon, the need for better data is paramount. The current reliance on manual review of inconsistent preprint forms is insufficient for a program of this scale. Policymakers must develop more robust, real-time reporting mechanisms to ensure that every dollar spent on Medicaid—whether base payment or state-directed supplemental—is being used to drive genuine, measurable improvements in patient health outcomes.
The transition period between now and the full implementation of the 2025 reconciliation law will be a litmus test for the relationship between federal oversight and state flexibility. If the goal is to reduce spending without sacrificing the health of the most vulnerable populations, the strategy must evolve from blunt fiscal cuts to more sophisticated, value-based payment reforms that prioritize patient care over administrative convenience.
In conclusion, the $137 billion currently flowing through State Directed Payments is more than just a line item in a budget; it is the financial backbone of the Medicaid managed care system. As that backbone faces a systematic restructuring, the challenge will be to ensure that fiscal discipline does not come at the cost of the nation’s public health infrastructure. The coming years will reveal whether the 2025 reconciliation law acts as a necessary correction or a catalyst for a decline in healthcare access for the millions of Americans who rely on Medicaid.