

By [Your Name/Editorial Desk]
In the landscape of oncology, the difference between a terminal diagnosis and a future defined by milestones—birthdays, graduations, and the quiet joy of daily life—often hinges on a single, pivotal decision. For Melinda Bachini, that decision came in April 2012, when she walked into the National Cancer Institute (NCI) not as a name, but as "Patient 3737."
While the designation might strike some as impersonal, for Bachini, that number was a tether to life. It represented her enrollment in a cutting-edge clinical trial—a last-ditch effort after standard medical protocols had failed to halt the progression of her stage IV cholangiocarcinoma, or bile duct cancer. Today, more than a decade later, Bachini stands not just as a survivor, but as a formidable advocate, reshaping how the world perceives the role of patients in scientific discovery. Her journey is a testament to the transformative power of clinical research and a clarion call to address the systemic barriers that keep life-saving innovations out of reach for the majority.
The Chronology of a Medical Odyssey
The trajectory of Bachini’s struggle began with a diagnosis that is notoriously difficult to treat. Cholangiocarcinoma is a rare, aggressive malignancy often discovered only when it has reached an advanced stage. By the time Bachini received her diagnosis, the tumor in her liver had engulfed the right lobe.
Initial surgical interventions provided a temporary reprieve, but the cancer was relentless, eventually metastasizing to her lungs. By early 2012, traditional chemotherapy had failed to yield long-term results, and her physical condition was deteriorating rapidly. "By 2012, my tumors were growing aggressively, and I could barely climb a few stairs without becoming breathless," Bachini recalls.
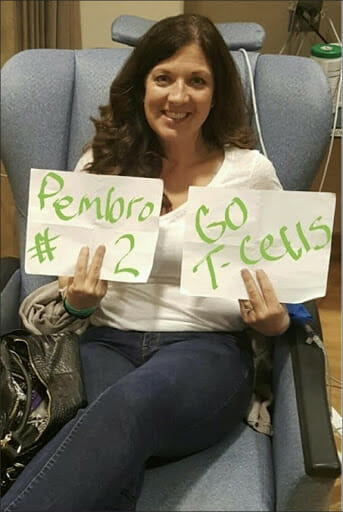
Driven by a mix of desperation and hope during a sleepless night spent reviewing medical bills, Bachini conducted an exhaustive online search that led her to Dr. Steven Rosenberg’s lab at the NCI. Dr. Rosenberg was pioneering "tumor-infiltrating lymphocyte (TIL) therapy," an experimental approach that extracts immune cells from a patient’s own tumor, expands them in a lab, and re-infuses them back into the body to mount a targeted attack against the cancer.
The process was grueling, involving invasive procedures and the uncertainty inherent in an unproven treatment for bile duct cancer. Yet, the alternative was surrender. Within six months of the therapy, her tumors showed significant regression, followed by another six months of stabilization. That trial did more than buy her time; it restored her quality of life and turned the tide against a disease that had been deemed insurmountable.
The Statistical Reality: Why Trials Remain Underutilized
Despite the life-altering potential of clinical trials, the medical community faces a persistent, troubling bottleneck: low participation rates. Data indicates that only 5% to 7% of adult cancer patients enroll in clinical trials. This figure remains stagnant despite overwhelming evidence that trials are the engines of progress in modern medicine.

The Myth of the "Last Resort"
A primary obstacle is the psychological barrier built on misinformation. Many patients view clinical trials as a "last resort" or fear that they will be treated as "guinea pigs." In reality, trials are the front line of innovation. They provide patients access to therapies that may be years away from mainstream availability.
Structural and Socioeconomic Hurdles
Beyond myths, the barriers to entry are systemic:
- Geographic Limitations: Many cutting-edge trials are concentrated at major academic medical centers, creating a "zip code lottery" where distance and travel costs preclude participation.
- Financial Disparity: Even when travel is possible, the secondary costs of lodging, time away from work, and caregiver support are prohibitive for many families.
- Knowledge Gaps: There is a significant deficit in the communication between clinicians and patients regarding the availability of trials, often due to a lack of time or specialized knowledge in the primary care setting.
Supporting Data: Bridging the Equity Gap
The data on disparities is stark. Patients from underrepresented communities, including racial and ethnic minorities and those from lower socioeconomic backgrounds, are disproportionately excluded from trials. This exclusion is not merely a matter of social justice; it is a scientific failure.
When trials do not reflect the diversity of the patient population, the resulting data may not account for genetic, environmental, or lifestyle factors that influence how a treatment works. By failing to include a broad spectrum of humanity in research, the scientific community misses critical insights necessary to develop universally effective therapies.
"We are missing critical data to address disparities," Bachini notes. "Without equitable access, we cannot develop more effective treatments that work for everyone, regardless of their background."
Official Perspectives: The Push for Systemic Change
Leading institutions and advocacy organizations, such as the Cholangiocarcinoma Foundation, are intensifying their efforts to dismantle these barriers. The consensus among medical leadership is that the paradigm must shift from "trial as a last resort" to "trial as a standard of care."
The Role of Advocacy
Organizations are now prioritizing "trial literacy"—educating both patients and providers about the benefits of early enrollment. By empowering patients to ask, "Is there a clinical trial for me?" at the point of diagnosis, the foundation aims to shift the narrative.
Policy and Industry Responsibility
Policymakers are being urged to incentivize the expansion of trial sites into community hospitals, reducing the travel burden on patients. Furthermore, pharmaceutical and biotech industries are under increasing pressure to provide financial stipends or logistics support for trial participants, ensuring that participation is not a luxury afforded only to the wealthy.
Implications for the Future of Healthcare
The shift from Patient 3737 to survivor and advocate represents a broader evolution in the doctor-patient relationship. In the modern era, the patient is no longer a passive recipient of care but an active partner in the scientific process.
The Power of Collaboration
When patients like Bachini engage in clinical research, they contribute to a "treatment blueprint" that benefits future generations. Every trial, whether it results in a cure or a refinement of current understanding, provides the data points necessary to turn cancer from a terminal diagnosis into a manageable chronic condition.
A Call to Action
The implications for the reader are clear: whether you are a patient, a caregiver, or a healthcare professional, you hold a piece of the puzzle. Challenging the stigma of clinical trials is an act of advocacy that can save lives.
"I urge every reader to learn more about clinical trials," Bachini says. "Join us in challenging the myths and ensuring every patient has access. Because no one should ever be just a number. And because every number has the potential to become a story of survival, like mine."
Conclusion: Turning Numbers into Narratives
The journey of Melinda Bachini serves as a profound reminder that the history of medicine is written in the blood and resolve of those who choose to participate in the unknown. As we look toward the future, the goal is clear: to democratize access to innovation.
We must move beyond the constraints of limited geographic access and financial inequality. We must dispel the myths that equate research with experimentation and replace them with the truth—that clinical trials are the most hopeful path forward. By fostering a culture of inclusion and urgency, the healthcare system can ensure that every patient, regardless of their status or location, has the opportunity to become more than a statistic. They have the opportunity to become a pioneer, and perhaps, a survivor.
As Bachini’s story proves, the difference between a tragic end and a long, full life can be found in a lab, in a protocol, and in the courageous act of saying "yes" to a clinical trial.







