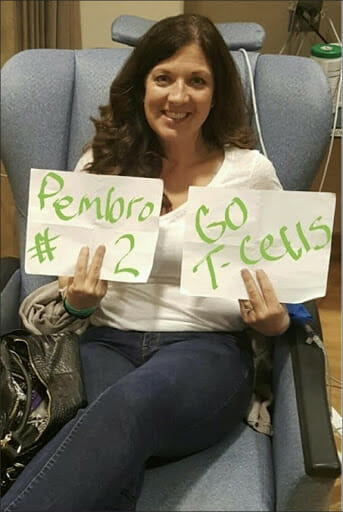
In the quiet, clinical corridors of the National Cancer Institute (NCI) in April 2012, Melinda Bachini was stripped of her name and assigned a designation: Patient 3737. To an outsider, the reduction of a human being to a four-digit string might feel cold, or even dehumanizing. But for Bachini, who had exhausted the standard arsenal of conventional oncology, that number was not a badge of insignificance—it was a lifeline.
Fifteen years later, Bachini is not merely a survivor; she is a grandmother, a wife, and a formidable patient advocate. Her journey is a testament to the life-changing potential of clinical trials—a realm of medicine often shrouded in fear, misconception, and underutilization. As she reflects on her transition from a terminal prognosis to a life reclaimed, she poses a challenge to the medical establishment and patients alike: it is time to dismantle the barriers preventing the next generation of survivors from accessing the cutting-edge therapies that saved her.
The Chronology of a Fight: A Patient’s Odyssey
The story of Melinda Bachini begins with a diagnosis that strikes terror into even the most resilient: cholangiocarcinoma, or bile duct cancer. It is a notoriously aggressive malignancy, frequently silent until it reaches Stage IV. By the time Bachini received her diagnosis, the tumor in her liver was so expansive it had consumed the right lobe.
The Initial Battle
Following the initial diagnosis, Bachini underwent surgery, a temporary measure that bought her precious time. However, the respite was brief. The cancer proved relentless, metastasizing to her lungs. Standard chemotherapy regimens failed to provide the long-term control required to keep the disease at bay. By 2012, the situation had become dire. Her tumors were proliferating aggressively, and the simple act of climbing a flight of stairs left her breathless—a chilling indicator of the disease’s encroachment on her respiratory capacity.
The Turning Point
The trajectory of her life shifted during a sleepless, anxiety-ridden night spent grappling with the mounting costs of her medical care. An exhaustive online search led her to the work of Dr. Steven Rosenberg, a pioneer in the field of immunotherapy at the NCI. Dr. Rosenberg’s team was exploring "tumor-infiltrating lymphocyte" (TIL) therapy—an experimental approach that, at the time, had not been proven for bile duct cancer.
The process was far from simple. It involved sequencing her tumor to isolate the specific immune cells capable of identifying and attacking the cancer. These cells were extracted, cultured and multiplied in a high-tech laboratory environment, and then re-infused into her body. The gamble paid off: for six months, her tumors showed clear regression, followed by another six months of complete stability. That trial did not just provide extra time; it restored her life.

Supporting Data: The Clinical Trial Paradox
Despite the success stories, the medical community faces a stark reality: participation in clinical trials remains alarmingly low. Data indicates that only 5% to 7% of adult cancer patients enroll in clinical trials. This figure stands in stark contrast to the vast number of patients who could potentially benefit from them.
Barriers to Entry
The reasons for this low participation rate are multifaceted, often interlocking to create an impenetrable wall for the average patient:
- Geographic Limitations: Many trials are concentrated in major urban research hubs, making them inaccessible for patients in rural or underserved areas.
- Systemic Misconceptions: A pervasive myth persists that clinical trials are a "last resort" for those with no other options, or that participants are being treated as "guinea pigs."
- Financial and Logistical Burden: Even when a trial is free, the ancillary costs—travel, lodging, and loss of income—often prove prohibitive for families already strained by medical bills.
- Lack of Awareness: Many patients and even primary care physicians are unaware of the trials available for specific, rare cancer subtypes, leading to missed windows of opportunity.
The "Last Resort" Myth
The narrative that trials are a final, desperate act is perhaps the most damaging of all. In reality, trials are the engines of medical progress. They are designed to answer complex scientific questions that refine care for the entire population. When a patient enrolls in a trial, they are not merely receiving a treatment; they are participating in the evolution of medicine. As Bachini notes, her own participation helped create a treatment blueprint that has since informed the care of countless others.
Official Responses and Systemic Equity
The medical establishment, including organizations like the Cholangiocarcinoma Foundation, is beginning to acknowledge that the "one-size-fits-all" approach to oncology is failing. The push for equity in clinical trials is no longer just a matter of social justice—it is a scientific necessity.
Addressing Health Disparities
Underrepresented communities are disproportionately excluded from trials due to historical mistrust, cultural barriers, and socio-economic inequities. This exclusion leads to a dangerous "data gap." If the demographic data of trial participants does not reflect the diversity of the patient population, the treatments developed may not be equally effective or safe for all groups.
The Role of Advocacy
As the Chief Patient Officer at the Cholangiocarcinoma Foundation, Bachini is at the forefront of policy reform. Her organization focuses on:
- Empowering Patients: Providing clear, accessible information so patients can advocate for themselves during consultations.
- Educating Providers: Ensuring that oncologists and primary care physicians view clinical trials as a primary treatment option rather than a secondary consideration.
- Policy Advocacy: Pushing for legislative changes that provide financial support for trial participation, such as covering travel expenses and expanding the geographic reach of research initiatives.
Implications: The Future of Cancer Care
The implications of expanding trial access extend far beyond the individual patient. We are currently in a golden age of immunotherapy and precision medicine, yet the pace of innovation is slowed by the slow accrual of participants.
From "Number" to "Narrative"
The transformation of "Patient 3737" into a voice for change underscores a fundamental truth: patients are not passive subjects. They are active partners in the research process. When a patient participates in a trial, they contribute data that might unlock a cure for the next generation. The shift from seeing a patient as a number to seeing them as a partner in discovery is essential for the future of oncology.
A Call to Action
The path forward requires bold, systemic action. Researchers must simplify the recruitment process, industry must invest in decentralized trial models that reach patients where they live, and policymakers must treat trial access as a fundamental component of patient care.
For the reader—whether a patient navigating a diagnosis, a caregiver supporting a loved one, or a citizen interested in the trajectory of public health—the message is clear: knowledge is the first line of defense. Challenging the myths surrounding clinical trials is not just an academic exercise; it is a vital step toward saving lives.
Melinda Bachini’s journey serves as both a beacon of hope and a call to arms. Her story proves that behind every statistic is a human life, and behind every clinical trial is the potential to turn a diagnosis into a story of survival. As she often says, no one should ever be just a number. Every number represents a unique life, and every life has the potential to redefine what is possible in the face of cancer. By breaking down the barriers to clinical trials, we do not just improve survival rates—we honor the humanity of every patient who walks through the doors of a research center, looking for a way forward.