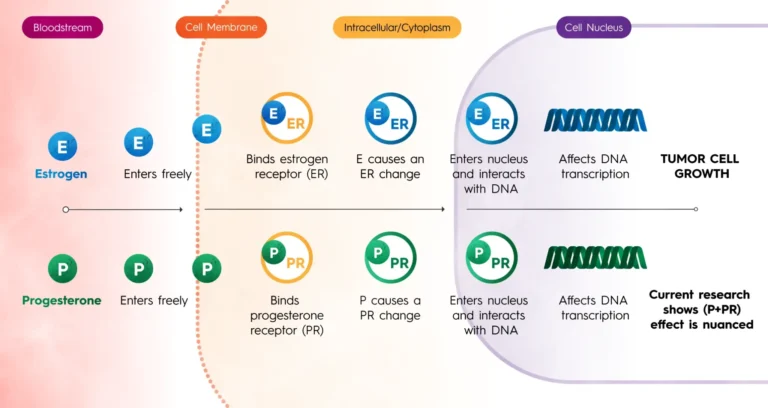
The landscape of breast cancer treatment has undergone a seismic shift over the last two decades. We have moved from a "one-size-fits-all" era, where radical surgeries and broad-spectrum chemotherapy were the standard of care, into the era of precision medicine. Today, a patient’s treatment plan is increasingly dictated by the microscopic and molecular details of their specific condition.
However, as the science becomes more sophisticated, so does the terminology. For many newly diagnosed patients, two terms—genetic testing and biomarker testing (often called genomic testing)—are frequently used interchangeably. While they both involve the study of DNA, they serve fundamentally different purposes in the oncology journey. Understanding these nuances is not merely an academic exercise; it is a vital step in ensuring patients receive treatment that is "smarter, not just stronger."
Main Facts: Defining the Two Pillars of Cancer Diagnostics
To navigate a breast cancer diagnosis, one must first distinguish between the DNA we are born with and the DNA within a tumor.
Genetic Testing: The Inherited Blueprint
Genetic testing, or germline testing, examines the DNA found in every cell of a person’s body. This is the genetic material inherited from one’s parents. The primary goal of this testing is to identify mutations—such as the well-known BRCA1 and BRCA2 genes—that significantly increase the lifetime risk of developing breast, ovarian, and other cancers.
Genetic testing answers the "Why?" and the "Who else?" It helps determine if a cancer diagnosis was driven by a hereditary predisposition and assesses whether family members might also be at an elevated risk.
Biomarker Testing: The Tumor’s "Personality"
Biomarker testing, also known as genomic or somatic testing, does not look at the patient’s healthy cells. Instead, it analyzes the specific genes within the cancerous tumor itself. These tests, such as Agendia’s MammaPrint and BluePrint, measure the activity of certain genes to predict how the cancer will behave.
Biomarker testing answers the "What now?" and "How aggressive?" It provides a molecular roadmap that helps oncologists determine the likelihood of recurrence and whether the patient will actually benefit from intensive treatments like chemotherapy.
Chronology: The Evolution of Breast Cancer Personalization
The journey toward personalized breast cancer care has evolved through several distinct phases:
The Era of Clinical Observation (Pre-1990s)
For much of the 20th century, treatment decisions were based almost exclusively on clinical factors: the size of the tumor, whether it had spread to the lymph nodes, and the age of the patient. If a tumor was large, the assumption was that it was aggressive, requiring aggressive treatment.
The Genetic Breakthrough (1994–1995)
The discovery of the BRCA1 and BRCA2 genes in the mid-1990s revolutionized the field. For the first time, clinicians could identify individuals at high risk before cancer even developed. This birthed the field of cancer genetics, allowing for preventative measures like increased screening and prophylactic surgeries.

The Genomic Revolution (2000s–Present)
By the early 2000s, scientists realized that two tumors could look identical under a microscope but behave entirely differently in the body. This led to the development of genomic profiling. In 2002, the 70-gene signature (MammaPrint) was developed to look deeper into the biology of early-stage breast cancer.
Today, the standard of care for Stage I and II breast cancer often involves these genomic assays to spare patients from the toxicity of chemotherapy when the molecular risk of recurrence is low.
Supporting Data: The Science Behind MammaPrint and BluePrint
The clinical utility of biomarker testing is backed by rigorous scientific data. Unlike traditional pathology, which describes what the cancer looks like, genomic testing describes what the cancer is doing.
MammaPrint: Assessing the Risk of Recurrence
MammaPrint is a genomic test that analyzes 70 genes most associated with cancer recurrence. The test categorizes patients into "Low Risk" or "High Risk" groups.
- The MINDACT Trial: A landmark study involving nearly 7,000 patients provided the definitive evidence for this test. It found that many women who were clinically "high risk" (based on tumor size or node status) but genomically "low risk" could safely skip chemotherapy without compromising their survival rates. This has spared thousands of women from the long-term side effects of chemo, such as neuropathy, heart damage, and cognitive "chemo-brain."
BluePrint: Identifying the Functional Subtype
While MammaPrint looks at the risk, BluePrint looks at the type. It analyzes 80 genes to determine the "functional subtype" of the breast cancer—Luminal, HER2-type, or Basal-type. This is crucial because traditional staining (IHC) can sometimes be ambiguous. BluePrint identifies the underlying "engine" driving the tumor’s growth, allowing doctors to choose the most effective targeted therapies.
Who Should Get These Tests?
According to clinical guidelines, biomarker testing is most beneficial for patients who:
- Are newly diagnosed with Stage I or II invasive breast cancer.
- Have a tumor size of 5cm or smaller.
- Are either lymph node-negative or have limited lymph node involvement (1-3 positive nodes).
- Need to decide if chemotherapy is a necessary addition to hormone therapy.
Official Responses: Perspectives from the Frontlines
The integration of these tests has been met with strong support from both the medical community and patient advocacy groups.
The Diagnostic Perspective:
Agendia, the developer of MammaPrint and BluePrint, emphasizes that "knowledge is power" in oncology. Their mission focuses on providing "actionable insights" that allow for a more nuanced approach to treatment. By focusing on the unique biology of each tumor, they argue that medicine becomes more efficient and more humane.
The Patient Advocacy Perspective:
Organizations like Sharsheret, which supports Jewish women and families facing breast and ovarian cancer, highlight the emotional and practical importance of these distinctions. For the Ashkenazi Jewish community, where the prevalence of BRCA mutations is 1 in 40 (significantly higher than the general population), genetic testing is often the first step.
"Patients often come to us confused by the sheer volume of data," says the advocacy community. "Distinguishing between genetic risk (what you might pass to your children) and biomarker results (what treatment you need tomorrow) is essential for mental clarity and informed decision-making."
The Clinical Perspective:
Oncologists increasingly view these tests as "tie-breakers." When a case is borderline, genomic data provides the confidence to either escalate treatment to save a life or de-escalate treatment to preserve the quality of life.
Implications: The Future of Personalized Oncology
The broader implications of distinguishing between genetic and biomarker testing extend into economics, ethics, and long-term survivorship.
1. De-escalation of Care
One of the most significant implications of biomarker testing is the "de-escalation" of treatment. Over-treatment is a major issue in early-stage breast cancer. By identifying patients who will not benefit from chemotherapy, the healthcare system reduces unnecessary costs and, more importantly, protects patients from the physical and emotional trauma of unnecessary toxic treatments.
2. Family Planning and Preventative Health
Genetic testing has implications that span generations. A positive BRCA result doesn’t just affect the patient; it informs their siblings, children, and cousins. It allows for a proactive approach to health that can stop cancer before it starts, shifting the focus from "sick care" to "well care."
3. Equity in Access
As these tests become the gold standard, a major challenge remains: ensuring equitable access. There is a growing push in the medical community to ensure that biomarker and genetic testing are covered by all insurance providers and available to patients in underserved communities, regardless of their socioeconomic status.
4. Treatment "Smarter, Not Stronger"
The mantra of modern oncology is to be as precise as a sniper rather than as broad as a carpet bomb. By using genetic testing to understand risk and biomarker testing to understand the tumor, the medical community can tailor interventions that maximize efficacy while minimizing collateral damage to the patient’s body.
Conclusion: Empowering the Patient
A diagnosis of early-stage breast cancer is a life-altering event that requires a series of rapid, complex decisions. However, patients do not have to navigate this path blindly. By understanding the difference between the genes they were born with (Genetic Testing) and the genes driving their tumor (Biomarker Testing), they can engage in a more meaningful dialogue with their medical team.
If you or a loved one is facing a new diagnosis, ask your oncologist:
- "Do I need genetic testing to see if this was inherited?"
- "Is my tumor a candidate for biomarker testing like MammaPrint or BluePrint?"
- "How will these results change my surgical or chemotherapy options?"
When treatment is based on individual biology, it moves beyond the statistics of the masses and focuses on the reality of the individual. In the fight against breast cancer, the most powerful weapon is not just the medicine itself, but the data that tells us how to use it.