The modern narrative surrounding obesity treatment has been dominated by a singular, pharmaceutical phenomenon: the rise of GLP-1 receptor agonists. With millions of Americans utilizing these medications for weight management and pharmaceutical giants like Eli Lilly vaulting to a $1 trillion market capitalization on the back of this demand, the prevailing public perception is that a “silver bullet” for the global obesity crisis has finally arrived.
However, beneath the surface of this blockbuster success story, a more nuanced and complex reality is emerging. Industry leaders, clinicians, and researchers are increasingly pushing back against the “one-size-fits-all” model, arguing that true metabolic health requires a departure from blockbuster drugs toward a more sophisticated, precision-based paradigm.
The Illusion of the Panacea
“I remember when we decided the internet was going to cure everything, and it didn’t—it came with a certain set of problems,” says Mark Bagnall, CEO of Phenomix Sciences. “GLP-1s are having a similar moment.”
While these drugs have been transformative for millions, they are not without their limitations. Data suggests that public enthusiasm is not perfectly aligned with clinical outcomes. A recent survey conducted by Phenomix found that only 33% of patients view GLP-1s as a definitive, long-term solution for their weight struggles. This skepticism is well-founded, as the clinical reality of these drugs involves significant hurdles, including inconsistent efficacy, high costs, and a host of potential side effects that are often under-communicated to patients.
A Chronology of the Obesity Treatment Shift
- Pre-2020: Obesity management is largely behavioral, focusing on diet and exercise with limited pharmacological support.
- 2021–2024: The "GLP-1 Revolution" takes hold. Semaglutide and tirzepatide become household names, driving massive consumer demand and unprecedented pharmaceutical market valuations.
- 2025: The number of Americans taking GLP-1s for weight loss crosses the 30 million mark. The World Health Organization (WHO) issues formal guidance, stressing that drugs must be part of a broader health strategy.
- 2026 and Beyond: Industry insiders shift focus toward the "post-GLP-1 era," prioritizing drug development pipelines that emphasize genetic markers and phenotypic classification.
The Reality of the Pipeline: Why Big Pharma is Hedging
If GLP-1s were truly the perfect panacea, the pharmaceutical industry would likely consolidate its efforts around them. Instead, the current landscape tells a different story. According to data from TD Cowen, over 160 obesity drugs were in active development by 2025, utilizing at least 68 distinct mechanisms of action.
“If you want one piece of evidence that drug companies don’t think GLP-1s are the panaceas, look at the pipeline,” says Bagnall. “There are 200 new drugs in development. Some are different versions of GLP-1s, some are not GLP-1s at all. The drug companies are telling us we’re going to need a lot of different solutions.”
This diversification is driven by the fact that obesity is not a monolith; it is a multifactorial condition driven by diverse biological, genetic, and environmental triggers. By investing in varied mechanisms of action, pharmaceutical firms are acknowledging that the next decade of metabolic care will require a portfolio of tools tailored to specific patient needs.
The Hidden Costs: Side Effects and Muscle Loss
The "silver bullet" narrative often obscures the medical trade-offs associated with rapid weight loss. While gastrointestinal distress—nausea, vomiting, and diarrhea—is the most commonly discussed side effect, more concerning trends have emerged regarding body composition.
An October 2024 review published in the American Heart Association’s journal, Circulation, highlighted a critical clinical concern: in many patients, a significant portion of the weight lost during GLP-1 therapy is muscle mass, not fat. For the general population, this is a health risk; for the elderly or those with underlying frailty, it is a dangerous development.
“You have to be really thoughtful, because there is a general health benefit to muscle mass—but at some point, if you’re already weak and older, now we go into a whole other category of issues: falls, broken bones,” Bagnall explains.
Beyond the physical toll, there is a financial one. Patients are increasingly paying out-of-pocket, not only for the high-cost medications themselves but for an additional $1,000 or more in secondary care to manage the side effects. For many, the experience of being promised a cure, only to face months of illness and stagnant results, leads to a cycle of disappointment that characterizes the current "failure" of the one-size-fits-all approach.
Official Guidance: The WHO Perspective
The World Health Organization has taken a firm stance, framing GLP-1s as merely one component of a comprehensive puzzle. In its 2025 guidelines, the WHO emphasized that medication alone cannot solve the global health crisis. Their recommendations highlight the necessity of integrating pharmacotherapy with:
- Structured, individualized nutritional plans.
- Regular, monitored physical activity.
- Continuous support from multidisciplinary healthcare teams.
The director-general’s sentiment is clear: medication is a tool to facilitate change, not a replacement for the fundamental pillars of metabolic health.
The Precision Medicine Frontier: Phenotypes and Genetics
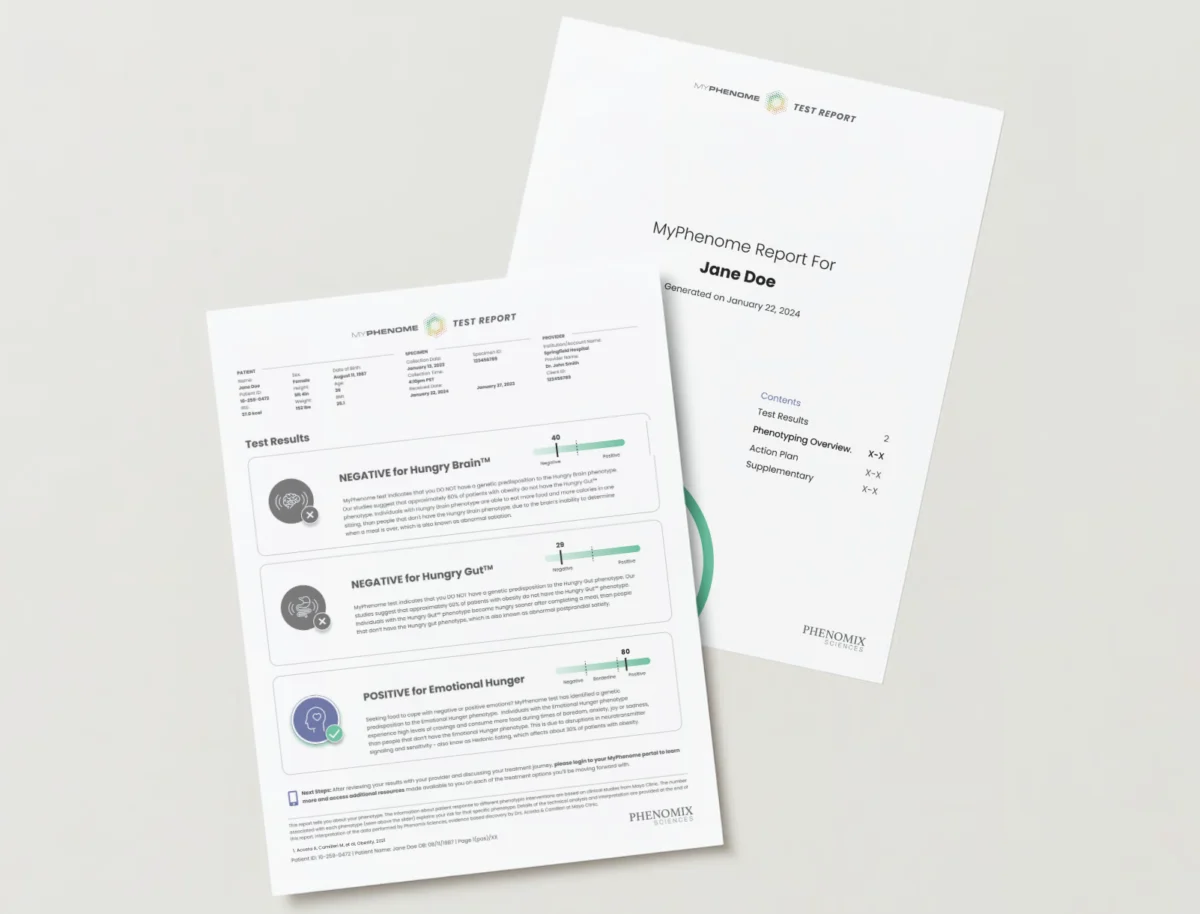
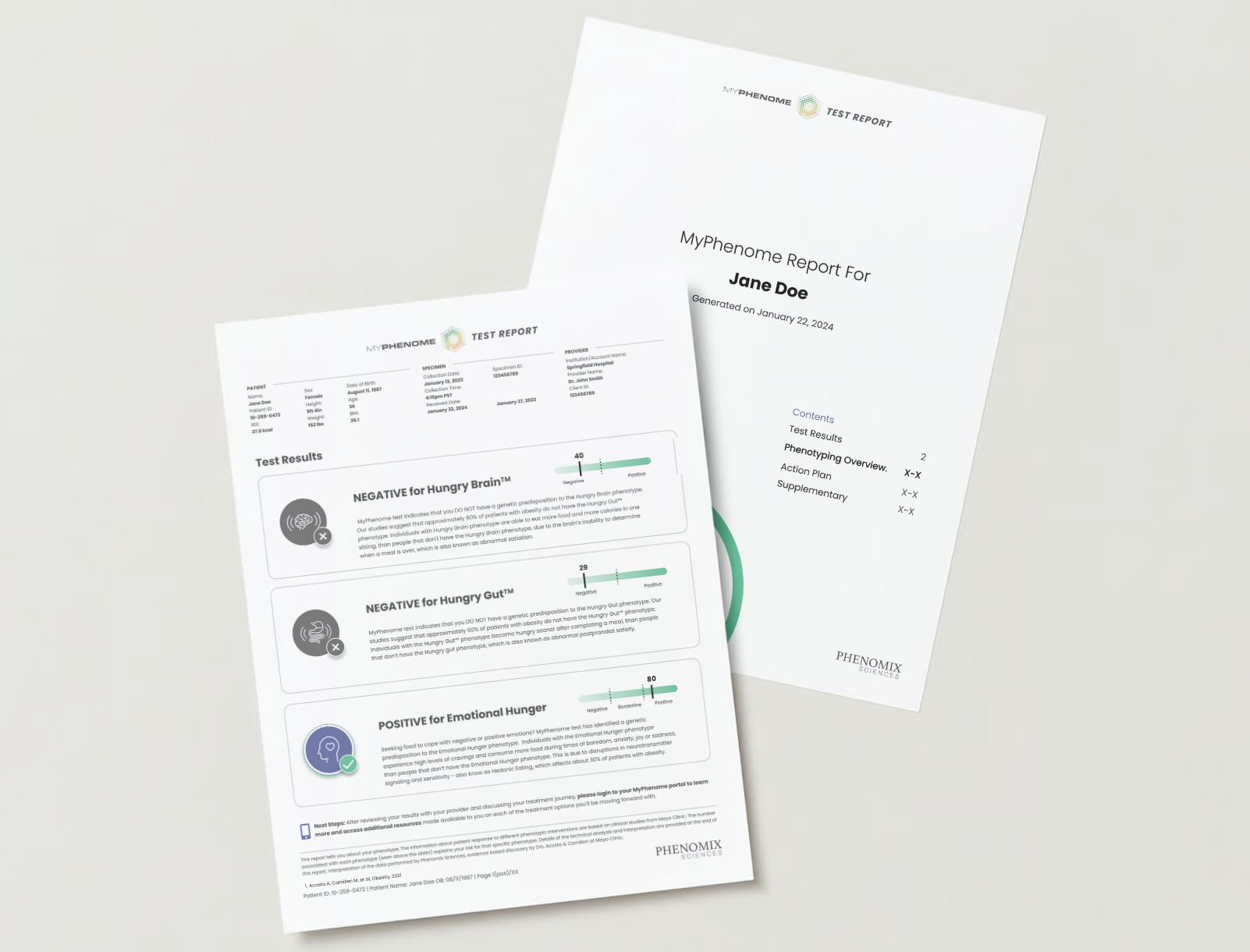
The future of obesity treatment lies in the same trajectory as oncology: moving from "trial-and-error" prescribing to molecular and genetic profiling. Phenomix Sciences is at the forefront of this shift, utilizing research from the Mayo Clinic to categorize obesity into four distinct phenotypes:

- Hungry Brain: Patients who struggle with constant hunger signals, often responding best to medications like phentermine or topiramate.
- Hungry Gut: Patients whose satiety signals are disrupted, making them ideal candidates for GLP-1 receptor agonists.
- Emotional Hunger: Patients driven by psychological triggers, often finding better success with combinations like Contrave.
- Slow Burn: Patients with an abnormally low metabolic rate, requiring different metabolic interventions.
Genetic factors account for 70% to 80% of a patient’s response to any given obesity drug. By testing for these specific phenotypes, clinicians can predict which patients will thrive on a specific drug and which will be “super-intolerant,” likely to suffer from severe side effects.
The "Oncology-Scale" Vision
The ambition of precision obesity medicine is to mirror the success of modern cancer treatment. Just as oncologists use genetic sequencing to choose the exact chemotherapy or immunotherapy agent for a specific tumor, future obesity specialists will use blood and genetic tests to map the patient’s metabolic profile before writing a single prescription.
"It’ll be like oncology, but on a mass scale," says Bagnall. The goal is to eliminate the "shotgun approach" to medicine, reducing the emotional and financial cost of failed treatments.
Implications for the Future
The implications of this shift are profound for patients, payers, and the pharmaceutical industry.
- For Patients: The move toward precision medicine promises shorter timelines to effective treatment and a significant reduction in the "despair" of ineffective therapies. It shifts the burden of care from the patient to the biology, providing a scientific explanation for why their weight loss journey may have been difficult.
- For Payers: Insurance providers, who currently struggle with the massive costs of covering GLP-1s for millions of users, may find that precision diagnostics provide a better ROI. By ensuring the right patient gets the right drug, they can reduce the waste associated with ineffective prescriptions and the long-term costs of managing secondary side effects.
- For the Pharmaceutical Industry: The next decade will likely see a thinning of the market for "general" weight loss drugs, replaced by a specialized landscape where companies compete based on the efficacy of their products for specific, well-defined genetic subtypes.
As the industry matures, the promise of "curing" obesity seems less like a fantasy and more like a reachable, albeit complex, scientific milestone. If Bagnall’s prediction holds—that we will have up to 50 targeted obesity drugs within a decade—we are moving toward an era where obesity is no longer viewed as a moral failing or a simple caloric imbalance, but as a manageable, phenotype-driven condition.
The silver bullet may not exist, but in its place, we are building something far more powerful: a complete medical arsenal.