By [Your Name/Editorial Desk]
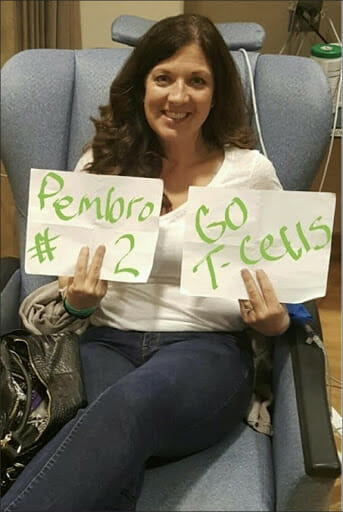
In the quiet corridors of the National Cancer Institute (NCI) in April 2012, Melinda Bachini was stripped of her identity and reduced to a digit: Patient 3737. At the time, the designation did not feel like a dehumanizing label; it felt like a lifeline. For Bachini, who had exhausted the standard arsenal of conventional oncology, that number represented a seat at the table of cutting-edge scientific innovation. Today, fifteen years later, Bachini is not merely a survivor—she is a grandmother, a wife, and a formidable Chief Patient Officer at the Cholangiocarcinoma Foundation, serving as a living testament to the transformative power of clinical trials.
Her story is more than a personal victory; it is a clarion call to the medical community, policymakers, and the public to rethink how we approach the "last resort" of clinical research.
A Chronology of Survival: From Diagnosis to Breakthrough
The trajectory of Bachini’s illness was, by all medical accounts, insurmountable. Cholangiocarcinoma—a rare and aggressive bile duct cancer—is frequently characterized by its late-stage presentation. By the time Bachini received her diagnosis, the disease had already claimed the right lobe of her liver.
The Precipice of Despair
Following an initial surgery that provided only temporary reprieve, the cancer metastasized to her lungs. Standard chemotherapy regimens, the bedrock of oncology, failed to halt the progression. By 2012, Bachini’s physical decline was marked by an inability to climb stairs without gasping for air. Trapped in a cycle of mounting medical debt and worsening prognosis, she took her fate into her own hands during a sleepless night of research. Her search led her to the work of Dr. Steven Rosenberg and his pioneering team at the NCI, who were experimenting with tumor-infiltrating lymphocyte (TIL) therapy.
The Scientific Frontier
The procedure was, by any definition, daunting. It involved extracting tumor samples, sequencing the genetic makeup of her specific cancer, identifying immune cells capable of attacking those tumors, and then "multiplying" those cells in a laboratory before re-infusing them into her body. It was an experimental frontier, a treatment protocol not yet validated for bile duct cancer. Yet, faced with the terminal nature of her condition, Bachini viewed the trial as the only logical next step.
The results were nothing short of miraculous: within six months, her tumors showed significant regression, followed by another six months of stability. The trial did not just grant her time; it restored her quality of life, allowing her to witness milestones she once thought she would never see.

Supporting Data: The Clinical Trial Participation Gap
Bachini’s journey highlights a systemic failure in oncology. Despite the potential for life-altering outcomes, only 5% to 7% of adult cancer patients participate in clinical trials. This statistic represents a critical bottleneck in the advancement of medical science.
Barriers to Entry
The reasons for this low participation rate are multifaceted and deeply entrenched:
- Geographic Limitations: Many trials are centralized at major research universities or national institutes, making them inaccessible to rural or low-income patients.
- The "Guinea Pig" Stigma: Persistent myths suggest that trial participants are mere subjects of experimentation rather than partners in progress.
- Lack of Physician Referral: Often, oncologists in community settings fail to discuss clinical trials as an early treatment option, relegating them to the "last resort" category.
- Financial and Logistical Burdens: The hidden costs of travel, lodging, and time away from work effectively exclude the working class and marginalized communities from participating in the very research that could save them.
The Cost of Inaction
When trial participation remains low, the "n" (sample size) of studies remains small. This slows the rate of scientific discovery, delays the FDA approval of new drugs, and limits our understanding of how different populations—particularly underrepresented minorities—respond to novel treatments. Without diverse participation, clinical data remains incomplete, perpetuating healthcare disparities that continue to claim lives disproportionately.
Official Perspectives and Expert Consensus
Medical researchers and advocacy groups are increasingly vocal about the need for a paradigm shift. Dr. Steven Rosenberg’s work at the NCI, which helped save Bachini, has long championed the idea that the immune system, if properly "taught," can be the most effective cancer-fighting tool.
A Call for Institutional Change
Experts argue that the responsibility for increasing trial participation rests on three pillars:
- Healthcare Providers: Physicians must be incentivized and trained to present clinical trials as viable treatment options at the time of diagnosis, not as a final option after all other therapies have failed.
- Policymakers: Legislative action is required to cover the costs associated with trial participation, such as travel and lodging, ensuring that socioeconomic status does not dictate survival.
- Industry and Research Sponsors: There is a mandate for decentralized trials. By leveraging digital health tools and local clinic partnerships, research can be brought to the patient, rather than requiring the patient to relocate to the researcher.
"Clinical trials are not just about testing a drug," says Bachini. "They are about answering the complex biological questions that accelerate the entire field of medicine. When a patient enters a trial, they are helping to build a blueprint that will save the person who receives the same diagnosis five, ten, or twenty years down the road."
Implications for the Future of Oncology
The implications of expanding trial access are profound. We are currently in a golden age of immunotherapy and precision medicine. If we can bridge the gap between patient and researcher, we can move from the "one-size-fits-all" chemotherapy model to a more tailored, effective approach to cancer care.
The Role of Patient Advocacy
The Cholangiocarcinoma Foundation and similar organizations are now at the forefront of this movement. By debunking the myths surrounding clinical trials, they provide patients with the agency to advocate for their own treatment plans. This shift—from passive patient to active participant—is perhaps the most significant change in modern medicine.
Challenging the System
True innovation requires a culture of radical transparency. Hospitals must be held accountable for their referral rates, and pharmaceutical companies must ensure their trials are inclusive of the populations most affected by the diseases they are studying. Equity in access is not just a moral imperative; it is a scientific necessity.
Conclusion: Every Number is a Story
Melinda Bachini’s story serves as a bridge between the sterile, cold world of medical data and the warm, human reality of life after cancer. Her journey from "Patient 3737" to a grandmother and advocate proves that clinical trials are not the end of the line—they are the beginning of a new chapter.
As we look toward the future of oncology, the goal is clear: we must dismantle the barriers that keep patients from these life-saving opportunities. We must replace fear with education and isolation with community. Because, as Bachini reminds us, no patient should ever be reduced to a number. Every number represents a human life, a family, and a potential story of survival waiting to be written.
The next time a doctor mentions a clinical trial, it should not be a sign of defeat. It should be seen for what it truly is: an invitation to join the front lines of a war that is being won, one patient at a time. The evolution of cancer treatment depends on the courage of those willing to step into the unknown, and it is the duty of society to ensure they have the path, the support, and the resources to do so.