By Jonathan Gardner
Published May 26, 2026
In a milestone that could redefine the standard of care for millions suffering from chronic cardiovascular disease, Eli Lilly and Company has announced promising clinical data for a novel base-editing therapy designed to provide a durable, one-time solution for lowering “bad” cholesterol. The data, unveiled at the European Atherosclerosis Society (EAS) Congress and simultaneously published in the New England Journal of Medicine, signals a successful leap forward in genetic medicine, clearing the path for a Phase 2 trial scheduled to commence by the end of 2026.
The Evolution of Cardiovascular Care
The treatment of cardiovascular disease has remained a cornerstone of modern medicine for the past four decades, yet it has been plagued by patient non-compliance and therapeutic ceilings. The history of cholesterol management began in earnest with the introduction of statins, such as Pfizer’s Lipitor, which revolutionized the prevention of heart attacks and strokes by inhibiting cholesterol synthesis in the liver.
Following the statin era, the industry saw the rise of PCSK9 inhibitors—antibody-based drugs like Repatha—which offered a more targeted approach to LDL (low-density lipoprotein) reduction. However, these therapies are far from a panacea. Statins are frequently associated with debilitating side effects, including myalgia and joint pain, leading many patients to discontinue treatment. PCSK9 inhibitors, while highly effective, require frequent injections and are often hampered by insurance access barriers and high costs.
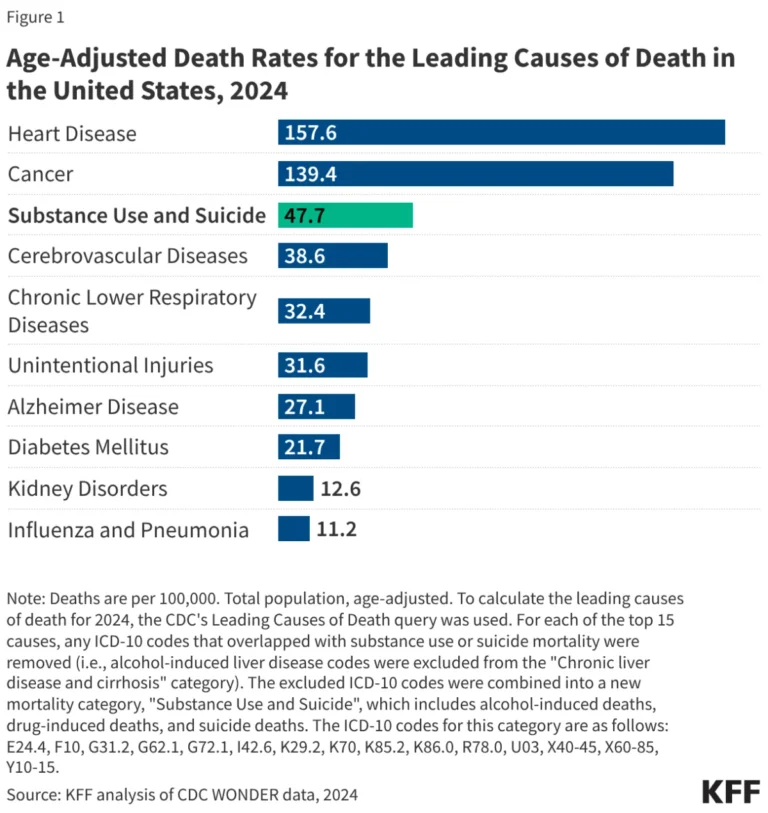
For the millions of patients whose LDL levels remain stubbornly high despite standard therapies, the clinical gap remains significant. "With coronary artery disease still one of the leading causes of death worldwide, the need for new approaches is real," noted Dr. Riyaz Patel, a cardiologist at Barts Health NHS Trust in London.

The Science of VERVE-102: Rewriting the Genetic Code
The therapy at the heart of this development, VERVE-102, represents a radical departure from traditional pharmacology. Rather than daily pills or periodic injections meant to sequester proteins or block enzymes, VERVE-102 utilizes base editing—a precision gene-editing technology—to permanently alter the genetic instructions within the liver.
By targeting the PCSK9 gene, which plays a pivotal role in regulating LDL metabolism, the therapy effectively "turns off" the production of the protein. The mechanism functions by changing a single nucleotide letter in the DNA sequence. This is a one-time intervention: once the gene is edited, the liver’s production of the PCSK9 protein is durably suppressed, theoretically offering a lifetime of protection against elevated LDL levels with a single infusion.
Chronology of a Breakthrough
The path to this week’s announcement has been characterized by meticulous clinical validation and strategic investment:
- Initial Discovery: Verve Therapeutics identified the potential for base editing to address cardiovascular risk by targeting the liver’s PCSK9 production.
- Strategic Acquisition: Recognizing the potential to dominate the metabolic disease space, Eli Lilly entered into a major partnership and acquisition agreement, committing $1 billion to acquire Verve’s cardiovascular pipeline.
- The Phase 1 Trial: Enrollment commenced for a cohort of 35 patients, testing six escalating dose levels ranging from 0.3 to 1 milligram per kilogram of body weight.
- May 25, 2026: Lilly releases preliminary safety and efficacy data, showing significant, dose-dependent reductions in both PCSK9 and LDL levels.
- May 26, 2026: Full findings are presented at the EAS Congress and published in the New England Journal of Medicine, confirming the drug’s biological activity and favorable safety profile.
- Late 2026: Eli Lilly plans to initiate the Phase 2 clinical study to further refine dosing and assess long-term efficacy.
Supporting Data: Efficacy and Safety Profile
The data released this week provides a robust foundation for the drug’s potential. In the study of 35 enrollees, the clinical results demonstrated a direct correlation between the dosage of VERVE-102 and the suppression of the target protein.
Specifically, the results indicated that PCSK9 levels were reduced by between 55% and 88% among participants. This dramatic reduction in the target protein led to a corresponding drop in LDL cholesterol levels, which fell between 9% and 62%.
Crucially, the safety profile appears favorable for a gene-editing intervention. Investigators reported no treatment-related adverse events that would halt the progression of the trial. The most common side effects cited by enrollees were limited to minor reactions at the site of infusion and temporary fatigue. All 35 participants completed the prescribed regimen, and notably, there were zero withdrawals from the trial—an indicator of high patient tolerance and satisfaction in the study environment.
Strategic Implications for Eli Lilly
For Eli Lilly, the success of VERVE-102 is more than just a scientific victory; it is a strategic maneuver to secure its status as the global leader in metabolic health. Lilly has already established itself as a titan in the market through its blockbuster obesity and diabetes portfolio. By integrating genetic medicine into its cardiovascular pipeline, the company is positioning itself to treat the root causes of metabolic syndrome rather than just managing the symptoms.
Industry analysts suggest that if VERVE-102 proceeds through the regulatory pipeline and reaches Phase 3 testing by 2035, it could fundamentally alter the market landscape. Should the drug prove durable and safe in larger, long-term studies, it could displace the current multi-billion dollar market for PCSK9 inhibitors and statins, transitioning the treatment of hypercholesterolemia from a chronic disease model to a curative one.
The Future of Genetic Medicine in Cardiology
The implications of this study extend beyond the specific drug itself. It serves as a proof-of-concept for the viability of base editing in systemic diseases. If the medical community can safely and effectively edit the liver to manage cholesterol, the door is opened for similar genetic interventions for other liver-driven metabolic disorders, such as hypertriglyceridemia or non-alcoholic steatohepatitis (NASH).
However, challenges remain. Regulatory bodies like the FDA will require extensive evidence regarding the long-term safety of permanent gene alteration, including the potential for "off-target" edits. Furthermore, the healthcare system will need to develop new economic models to support the reimbursement of a "one-and-done" therapy, which carries a high upfront cost but offers substantial long-term savings by preventing expensive cardiac events.

As the industry looks toward the Phase 2 trial starting later this year, the scientific community remains cautiously optimistic. Dr. Patel’s sentiments reflect the broader mood: the status quo for heart disease treatment is insufficient, and the transition toward genetic precision medicine offers the first real hope for a permanent shift in how we prevent the world’s leading cause of death.
For now, Lilly’s data provides a compelling case that the future of cardiology may not be found in a pill bottle, but in the precise, permanent editing of our own biological instructions.