As the landscape of American healthcare undergoes a significant transformation, the implementation of the 2025 reconciliation law looms as a critical milestone for state Medicaid programs. Starting January 1, 2027, states will be required to condition Medicaid eligibility for the Affordable Care Act (ACA) expansion population—and those in specific waiver programs like Georgia and Wisconsin—on compliance with federal work requirements.
However, a central pillar of this legislation is the protection of vulnerable populations. The law mandates exemptions for those deemed "medically frail" or those with significant health needs. With the Centers for Medicare and Medicaid Services (CMS) set to issue formal interim final rules by June 1, 2026, state administrators are currently in a high-stakes race against time, balancing system infrastructure updates with the legal requirement to ensure that those who cannot work due to illness are not unfairly stripped of their coverage.
Main Facts: The Intersection of Eligibility and Health
The 2025 reconciliation law marks a departure from previous Medicaid policies by codifying work requirements as a condition of eligibility. Under these rules, able-bodied adults must prove participation in work or community engagement activities. Recognizing that a broad mandate could disproportionately harm those with serious health conditions, Congress included a "medical frailty" exemption.
The legal definition of "medically frail" is intentionally broad to encompass a wide spectrum of health challenges. It includes:
- Individuals who are blind or disabled.
- Those with physical, intellectual, or developmental disabilities that impair the performance of activities of daily living (ADLs).
- Individuals suffering from substance use disorders (SUD) or disabling mental health disorders.
- Patients with "serious or complex" medical conditions.
To minimize the administrative burden on patients—who are often already navigating complex healthcare systems—the law directs states to use existing data to verify eligibility where possible, rather than forcing individuals to navigate repetitive, document-heavy bureaucratic processes.
Chronology: A Tight Timeline for Implementation
The implementation of this policy is governed by a compressed schedule that leaves little room for error.
- January–March 2026: States conduct internal surveys and begin drafting operational frameworks for the medical frailty exemption.
- May 1, 2026: Nebraska becomes the first state to launch a model for these work requirements, providing a test case for the rest of the nation.
- June 1, 2026: The federal government’s mandatory deadline for CMS to issue an interim final rule. This document is expected to harmonize state efforts and provide the definitive legal standards for exemptions.
- January 1, 2027: The federal deadline for full, mandatory implementation of the work requirements across all states covered by the reconciliation law.
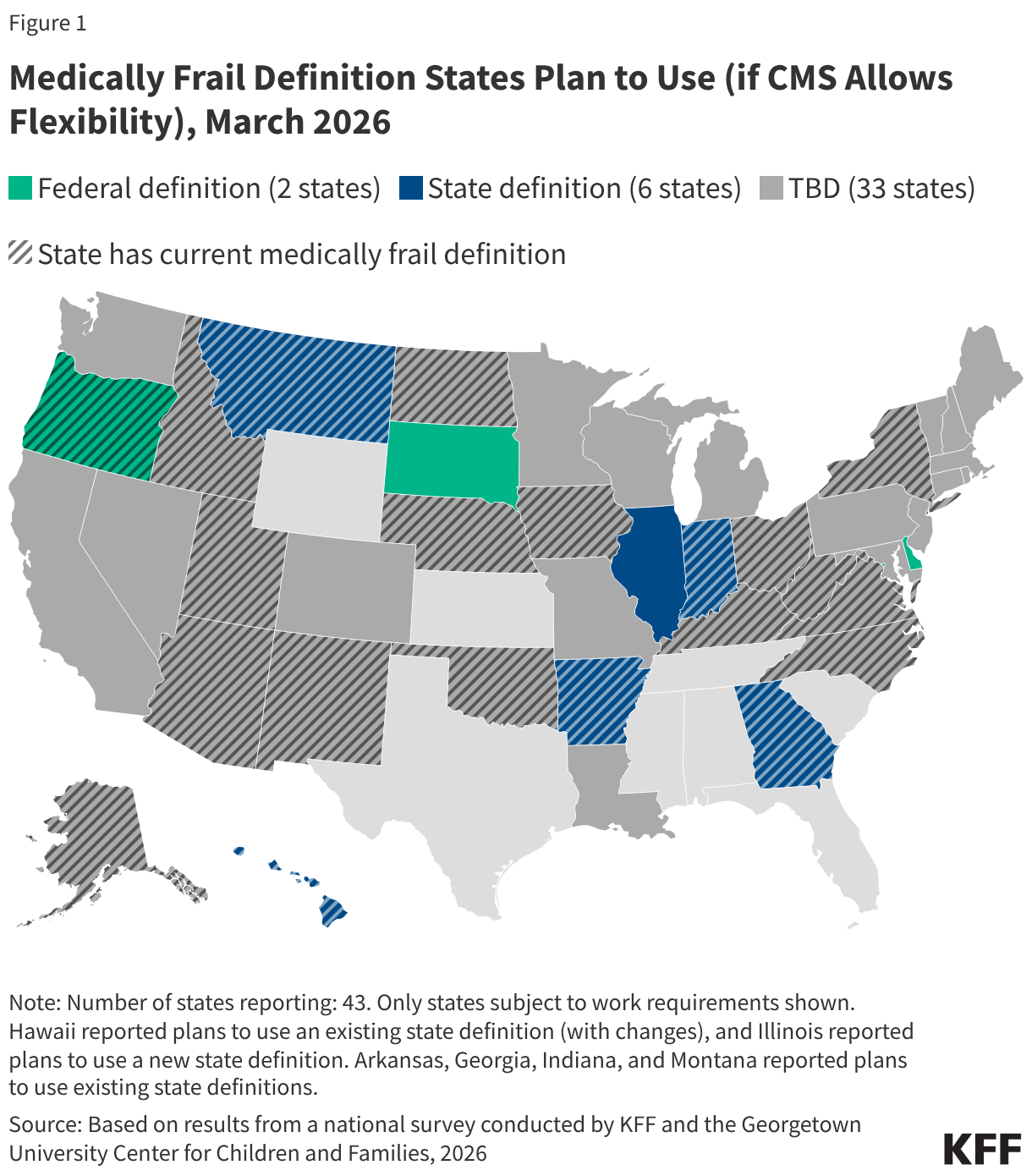
Supporting Data: How States Are Preparing
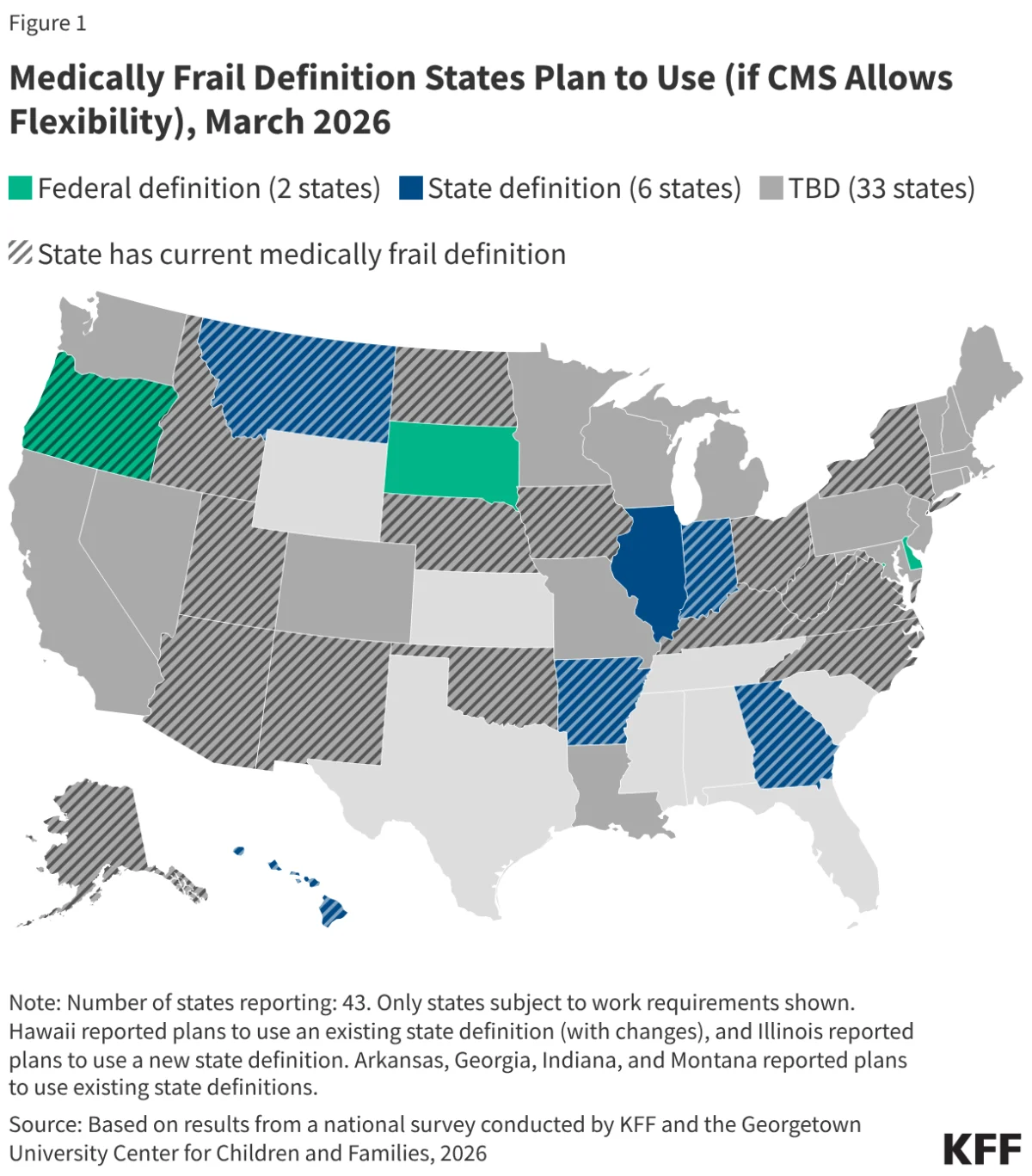
Recent surveys conducted by KFF underscore a landscape characterized by uncertainty. As of March 2026, approximately 22 states reported having an existing definition of medical frailty. However, because these definitions were largely developed for internal state-level program administration rather than federal work requirements, they may prove inadequate under the new law.
Data shows a stark divide in state strategy:
- Claims Data Utilization: 32 states intend to use existing Medicaid claims data to automatically flag medically frail enrollees, reducing the burden of proof on the individual.
- The Self-Attestation Debate: While 30 states express a desire to allow applicants to self-attest their medical frailty status in the absence of digital records, there is significant pushback. States like Arkansas, Hawaii, Indiana, and Montana have indicated they will not accept self-attestation, while North Carolina and Utah have passed legislation explicitly banning it.
Official Responses and State-Level Case Studies: The Nebraska Model
Nebraska’s early move to implement these requirements serves as a vital case study for the rest of the country. By publishing an index of diagnosis and procedure codes, Nebraska has provided a roadmap for how to categorize "medically frail" conditions.
The Nebraska Department of Health and Human Services (DHHS) is currently reviewing claims data to "auto-exempt" patients. If a patient’s medical records—which include codes for cancer, HIV, diabetes, and heart disease—are present, the system automatically tags them as exempt.
For those who do not show up in the claims data, Nebraska utilizes a "self-declaration form." While this is a step toward ease of access, critics note that the lack of automated verification for newer enrollees creates a "coverage gap" where individuals may lose benefits if they fail to navigate the paper-based declaration process correctly. Nebraska officials have stated their intention to transition to more automated verification as the system matures and as federal guidance becomes more crystallized.
The Role of CMS and Key Issues to be Addressed
The upcoming CMS guidance is the most anticipated document in the Medicaid administration sector. Because many states have already invested heavily in software and staffing based on preliminary, informal communications, any shift in the June 1, 2026, final rule could lead to significant budgetary and operational strain.
Defining Medical Frailty
The primary tension lies in how much flexibility states will have to define "medically frail." If CMS creates a rigid federal definition, states with broader, more inclusive existing definitions may be forced to scale back their protections. Conversely, if the definition is too loose, it could lead to inconsistent standards across state lines, undermining the intent of the federal law.
Verifying Medical Frailty
Verification remains the "Achilles’ heel" of the program. The key issues CMS must address include:
- The Reliability of Claims Data: How should states handle individuals who are medically frail but have not visited a doctor recently? If their claims data is outdated, they may be erroneously classified as "able-bodied."
- Standardizing Self-Attestation: Will CMS mandate that states accept self-attestation to protect the most vulnerable, or will they defer to state-level legislation that bans it?
- Cross-Program Data Sharing: Can states legally and technically integrate data from behavioral health managed care plans or Home and Community-Based Services (HCBS) programs to streamline the exemption process?
Implications: The Human and Economic Cost
The implications of these policies are profound. For the individuals enrolled in Medicaid, the process of verifying a disability or a chronic condition can be an exhausting endeavor, often requiring cooperation from doctors who are already stretched thin. If the system is too complex, the most vulnerable—those with mental health struggles or those who are homeless—risk losing their coverage due to administrative hurdles, not because they are non-compliant.
From an economic perspective, the cost of implementing these verification systems is non-trivial. States are investing millions in IT infrastructure, data analytics, and case management staff to handle the influx of documentation. If the system is not efficient, the administrative costs of enforcing work requirements could potentially exceed the savings generated by removing individuals from the rolls.
Furthermore, the "patchwork" approach—where a resident’s eligibility depends heavily on which state they live in—challenges the equity of the Medicaid program. A patient with a chronic, disabling condition might be automatically exempt in one state but forced to navigate a lengthy appeals process in another.
Conclusion: A Delicate Balance
As the June 1, 2026, deadline approaches, the nation watches to see how CMS will resolve the friction between administrative efficiency and the preservation of the safety net. The success of the 2025 reconciliation law will not be measured solely by the number of people entering the workforce, but by the integrity with which the system protects those who, by virtue of their health, cannot.
States are clearly attempting to act in good faith, balancing the mandate of the law with the logistical realities of their populations. However, the path forward requires a clear, decisive federal framework that prioritizes patient stability over procedural rigidity. Until then, the state of Medicaid remains in a state of flux, with millions of lives hanging in the balance of a bureaucratic transition.